


He was the go-to sports guy in DC. A masterful surgeon with countless academic publications, he trained orthopaedic surgeons worldwide and was the top physician for professional sports teams and Olympians.
Dr. Benjamin Shaffer had it all.
Yet Ben was more than a stellar surgeon. He was a kind, sensitive soul who could relate to anyone_—from inner city children to Supreme Court justices. He was gorgeous and magnetic with a sense of humor and a zest for life that was contagious. Patients came to him in pain and left his office laughing. They called him “Dr. Smiles.”
Ben was at the top of his game when he ended his life. So why did he die?
Underneath his smile, Ben hid a lifetime of anxiety. Recently weaned off anxiolytics, he was suffering from rebound anxiety and insomnia—sleeping just a few hours per night and trying to operate and treat patients each day. Then his psychiatrist retired and passed him on to a new one.
Days before he died, his psychiatrist prescribed two new drugs that worsened his insomnia and anxiety resulting in paranoia. He was told he would need medication for the rest of his life. Devastated, Ben told his sister it was “game over.”
Ben admitted he was suicidal with a plan though he told his psychiatrist he wouldn’t act on it. Ben knew he should check himself into a hospital, but was panicked. He was terrified he would lose his patients, his practice, his marriage, and that everyone in DC—team owners, players, patients, colleagues—would find out about his mental illness and he would be shunned.
Ben requested the remainder of the week off to rest. His colleagues were supportive, yet he was ashamed. He slept that night, but awoke wiped out on May 20, 2015. After driving his son to school, he came home and hanged himself on a bookcase. He left no note. He left behind his wife and two children.
I feel a kinship with Ben because I’m a cheerful doctor who was once a suicidal physician. I thought I was the only one—until I found myself at the memorial for our third doctor suicide in my small town. Despite his public death, nobody uttered the word suicide aloud. Everyone kept whispering “Why?” So I started counting doctor suicides. Within a few minutes I counted 10. Five years later I had a list of 547. By January this year, I had 757 cases on my registry. As of today that number is 1,013.
High doctor suicide rates have been reported since 1858 (1). Yet 160 years later the root causes of these suicides remain unaddressed. Physician suicide is a global public health crisis. More than one million Americans lose their doctors each year to suicide—_just in the US (2).
Of these 1,013 suicides, 888 are physicians and 125 are medical students. Surgeons have the greatest number of suicides on my registry, then anesthesiologists. (3)
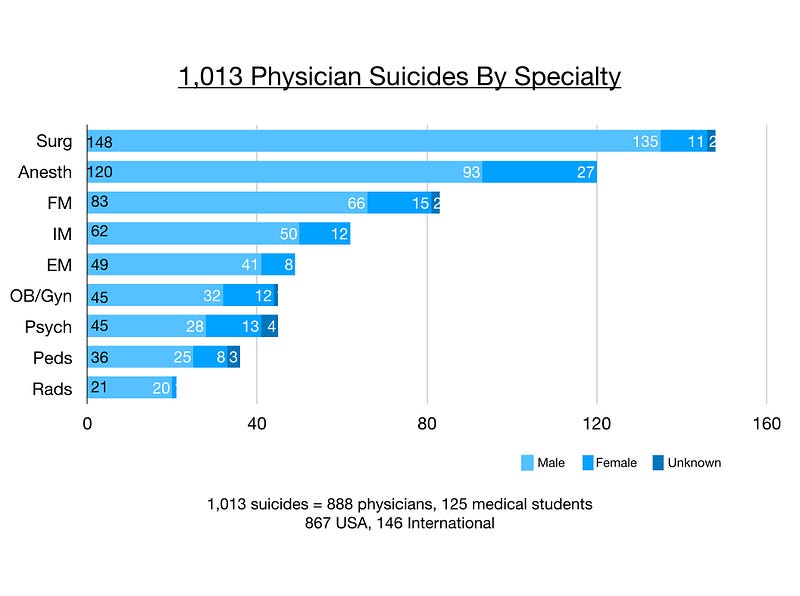
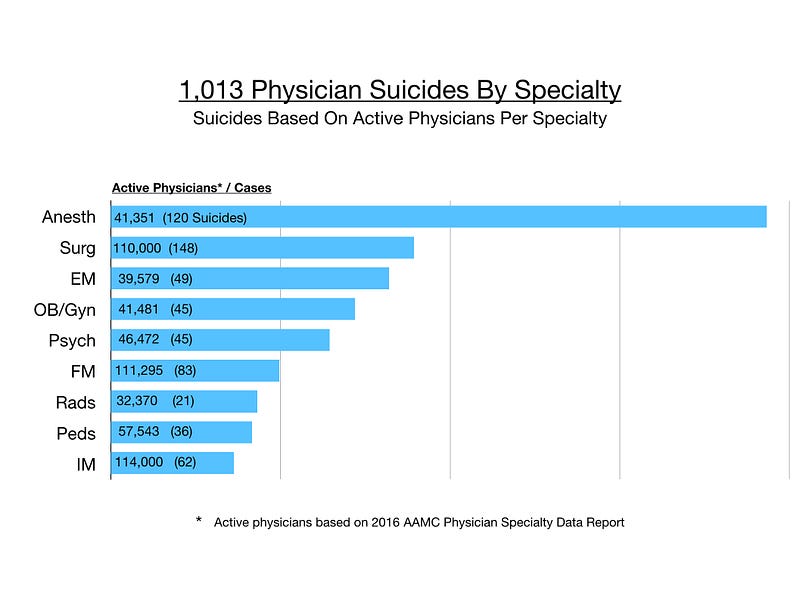
However when accounting for active physicians per specialty, anesthesiologists are more than twice as likely to die by suicide than other physicians. Surgeons are number two. (4)
 Graph by Dr. Wible
Graph by Dr. Wible
Doctor suicides on the registry were submitted to me during a six-year period (2012–2018) by families, friends, and colleagues. After speaking to thousands of suicidal physicians on my informal doctor suicide hotline and analyzing registry data, I’ve discovered surprising themes_—many unique to physicians.
Public perception maintains that doctors are successful, intelligent, wealthy, and immune from the problems of the masses. To patients, it is inconceivable that doctors would have the highest suicide rate of any profession (5).
Even more baffling, “happy” doctors are dying by suicide. Just back from Disneyland, just bought tickets for a family cruise, just gave a thumbs up to the team after a successful surgery—and hours later they shoot themselves in the head.
Physicians are masters of disguise and compartmentalization.
Yet students enter medical school with their mental health on par with or better than their peers. Suicide is an occupational hazard in medicine. Doctors develop on-the-job PTSD—especially in emergency medicine. Patient deaths—even with no medical error—may lead to self-loathing. Suicide is the ultimate self-punishment. Humans make mistakes. When doctors make mistakes, we’re publicly shamed in court and the media. We suffer the agony of harming someone else—unintentionally—for the rest of our lives
Blaming doctors increases suicides. Words like “burnout” and “resilience” are employed by medical institutions to blame doctors while deflecting accountability for inhumane working conditions in failing health systems. When punished for occupationally induced mental health wounds, doctors become even more desperate.
If physicians do seek help, they risk being disciplined. Doctors rightfully fear lack of confidentiality when receiving mental health care as private conversations could be turned over to medical boards and illegally accessed by supervisors via electronic records at their institutions. So physicians drive out of town, pay cash, and use fake names to hide from state boards, hospitals, and insurance plans that interrogate doctors about their mental health and may prevent or delay state licensure, hospital privileges, and health plan participation.
Doctors choose suicide to end their pain (not because they want to die). Suicide is preventable if we stop the secrecy, stigma, and punishment. In absence of support, doctors make impulsive decisions to end their pain permanently. I asked several male physician suicide survivors, “How long after you decided to kill yourself did you take action—overdose on pills or pull the trigger?” The answer: 3 to 5 minutes.
Ignoring doctor suicides leads to more doctor suicides. Let’s not wait until the last few minutes of a doctor’s life when heroic interventions are required. Most physician suicides are multifactorial involving a cascade of events that unfold months to years prior. So reach out to “happy” doctors today—_especially male anesthesiologists and surgeons who are least likely to cry or ask for help.
This post originally appeared at IdealMedicalCare.
References
2. Wible, P., 2014. “When doctors commit suicide, it’s often hushed up.” Washington Post.
3. Wible, P. Keynote, 19th Annual Chicago Orthopaedic Symposium, 8/18/18
4. AAMC Physician Specialty Data Report. 2016.
5. American Psychiatric Association (APA) 2018. Abstract 1–227, presented May 5, 2018.




