Clinical History:
A 28 year old woman presented with palate ulcer, which was biopsied.
Histopathology Images:
Diagnosis:
Necrotizing sialometaplasia
Test question (answer at the end):
Which of the following sites is most commonly involved in necrotizing sialometaplasia?
A. Dorsal tongue
B. Palate
C. Retromolar trigone
D. Submandibular gland
Discussion:
Necrotizing sialometaplasia (NSM) is a reactive, self limiting, salivary gland lesion, first described in 1973 by Abrams et al. (Cancer 1973;32:130). NSM is an important condition because the clinical and the histologic differential diagnosis includes benign and malignant entities. When misdiagnosed as a malignancy, it has the potential to result in overly aggressive surgical treatment. NSM is relatively uncommon, which can further compound the diagnostic dilemma since differential diagnostic considerations of rare diagnoses may be overlooked.
The most commonly proposed etiology for NSM is ischemic insult. A variety of factors are associated with NSM, such as local trauma (surgical, intubation-extubation, poorly fitting dentures, etc.), administration of local anesthetic, alcohol, smoking and cocaine use, external beam radiation and bulimia, and have the potential for contributing to ischemia. Occasionally, systemic diseases such as sickle cell disease, Buerger’s disease, Raynaud’s disease and HIV-AIDS have been linked to NSM (Oral Surg Oral Med Oral Pathol 1991;72:317, J Korean Assoc Oral Maxillofac Surg 2015;41:338). NSM affects a wide age range with a predilection in middle age and often a higher incidence in males than in females (Arch Pathol Lab Med 2009;133:692).
In most cases, NSM presents as a unilateral, isolated, nonhealing ulcerative lesion at the posterior hard palate or at the junction of the hard and soft palate. Less commonly, the surface mucosa is intact with a resulting mass-like clinical appearance. 10 - 15% of cases occur as synchronous, bilateral ulcerations on the palate (Oral Surg Oral Med Oral Pathol 1991;72:317). NSM may present in unusual locations including nasal cavity, trachea, larynx, maxillary sinus and major salivary glands (Arch Pathol Lab Med 2009;133:692).
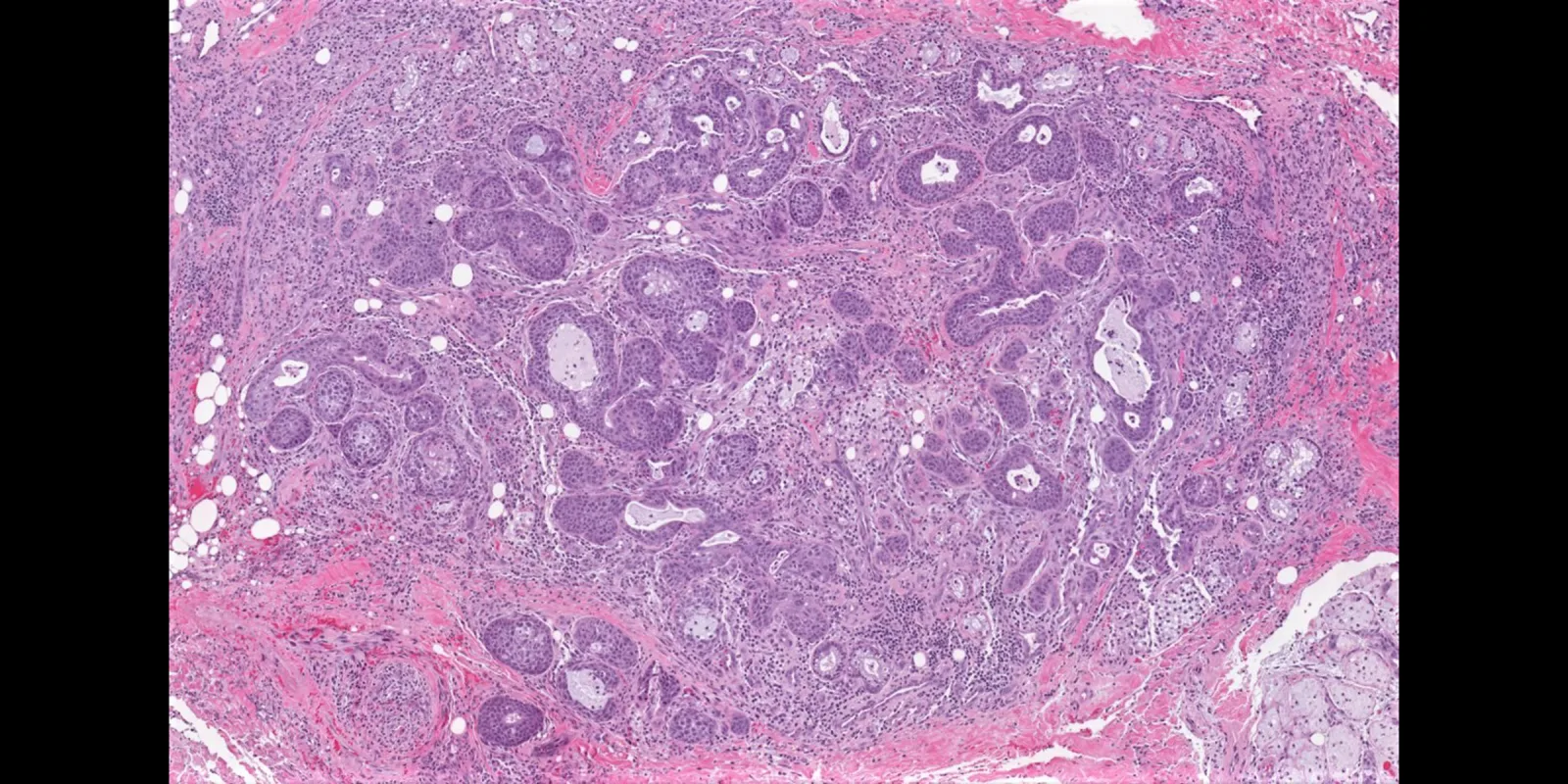
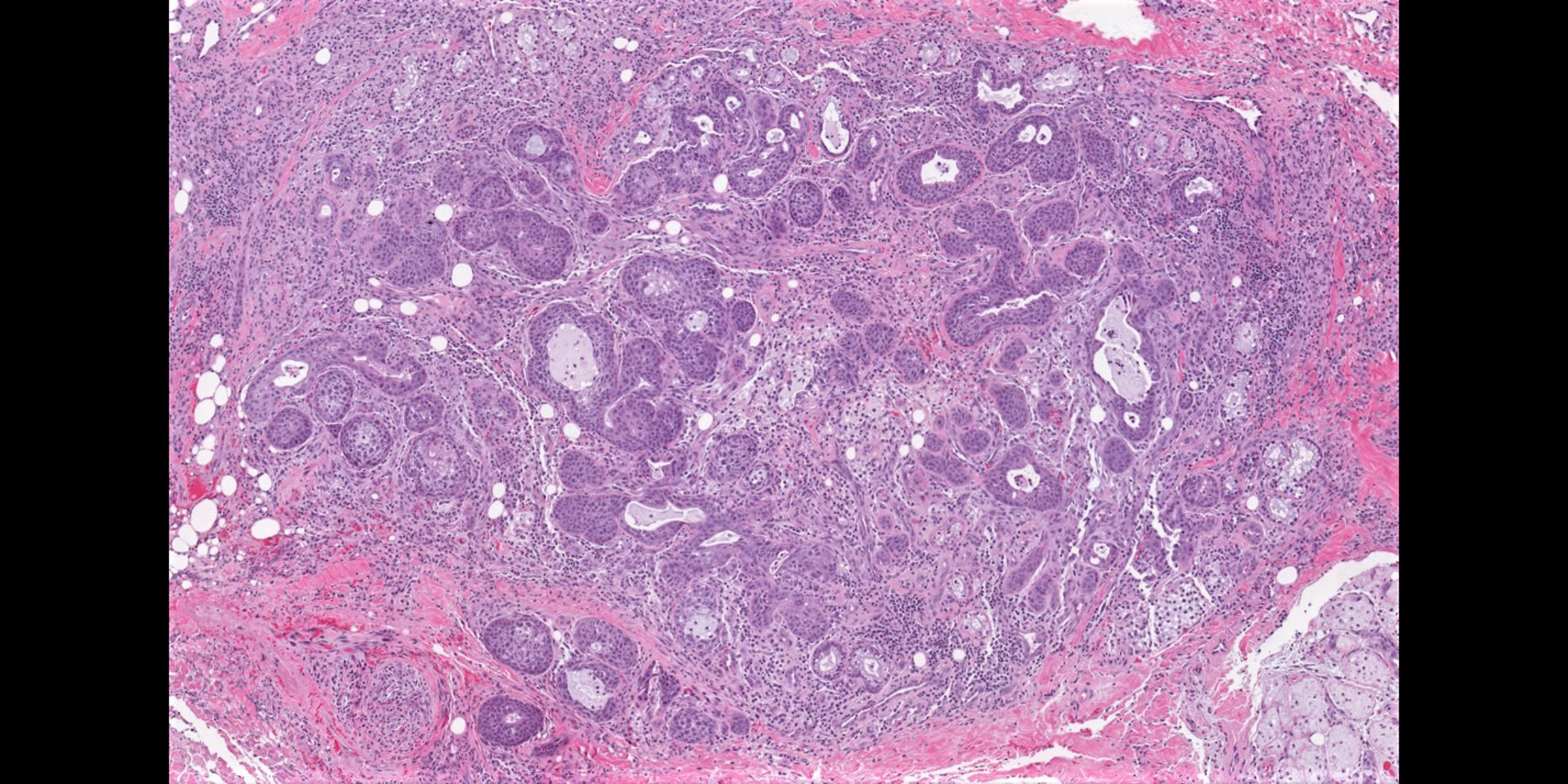
A spectrum of histologic changes is described but may not be found in every case and may be dependent on the age of the lesion and the biopsy sampling limitations (Cancer 1973;32:130, Histopathology 2007;51:184, BMC Oral Health 2020;20:206, Arch Pathol Lab Med 2009;133:692,Oral Surg Oral Med Oral Pathol 1991;72:317):
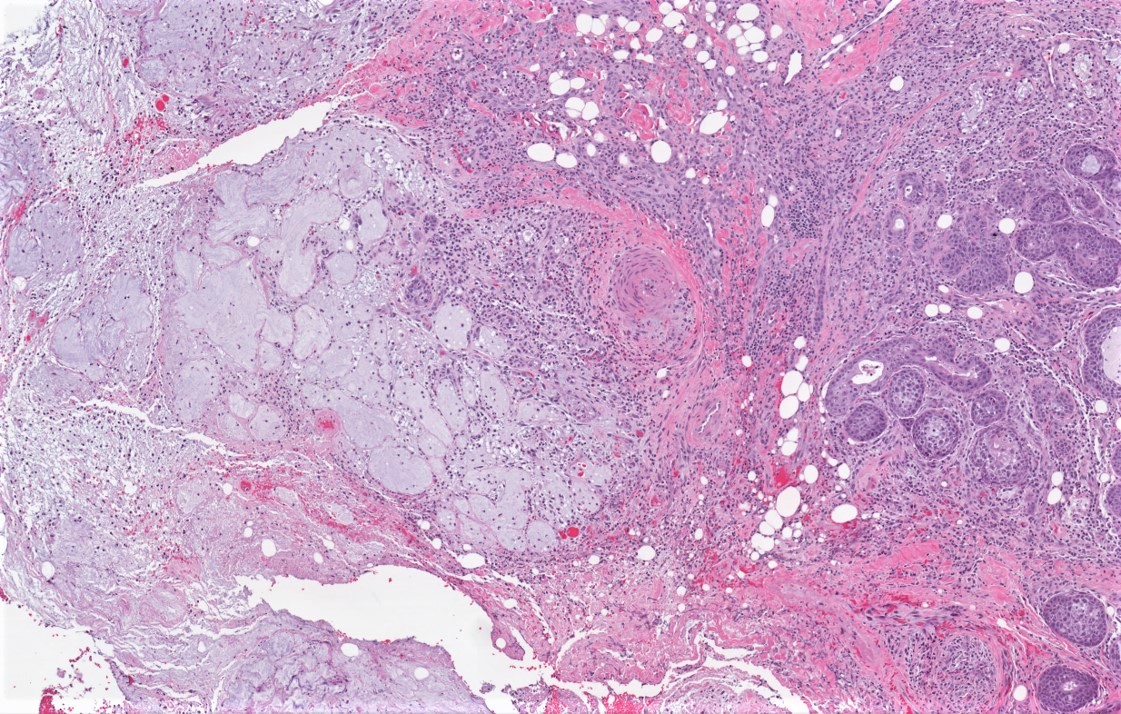
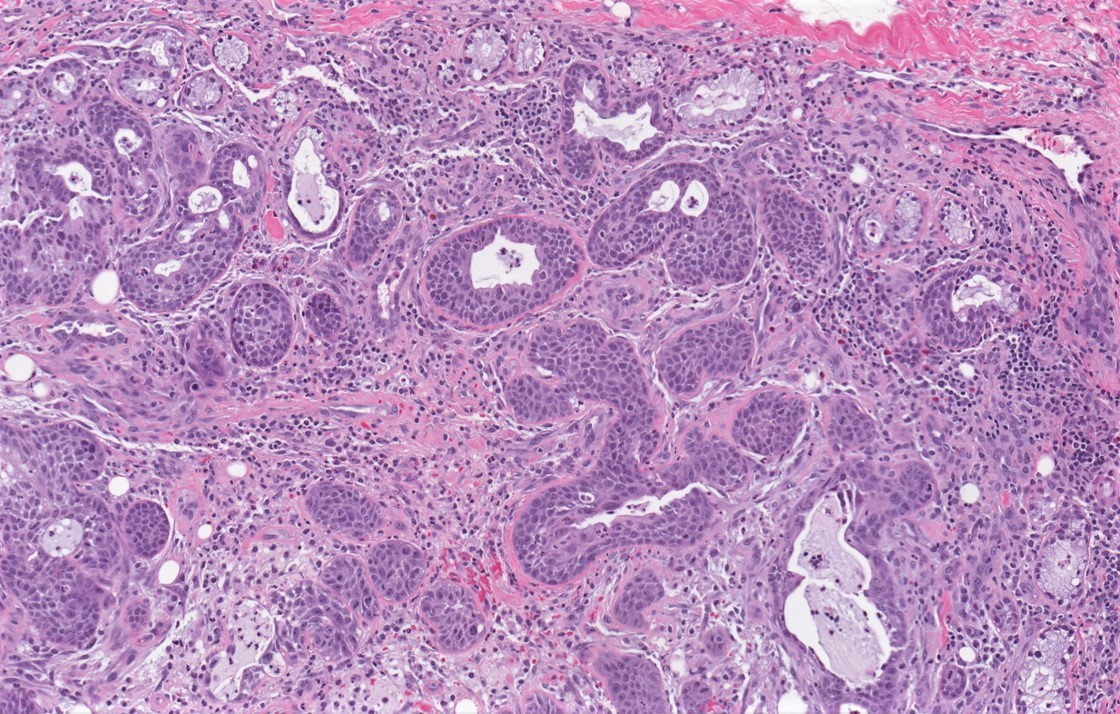
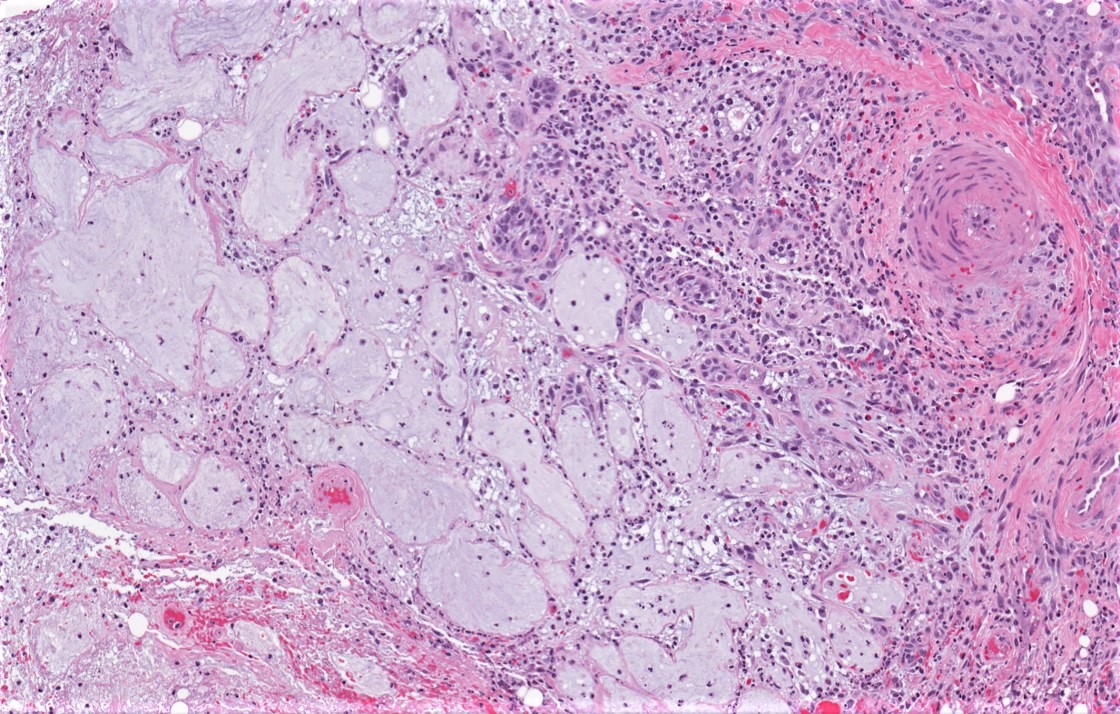
- Lobular necrosis or infarction of seromucinous glands with or without mucin spillage. Coagulative necrosis of salivary lobules may be a dominant feature in early lesions. There are small acini sized pools of mucin, surrounded by thin, necrotic septa and frequently ringed by neutrophils. Mucin pools may coalesce and extend into the adjacent tissue and elicit an inflammatory reaction.
- Squamous metaplasia of the ducts and acini. Ducts may contain mucin, acute inflammation or necro-inflammatory debris.
- Histologically bland nuclear morphologic features. The epithelial atypia expected in regenerating epithelium is possible but more often is limited to finding apoptotic cells and mitoses present, particularly in areas of inflammation. NSM secondary to radiation therapy may show radiation associated nuclear atypia. However, such atypia is typically randomly located in all types of cells, e.g. fibroblasts, squamous epithelium, squamous metaplasia, ductal and myoepithelial cells.
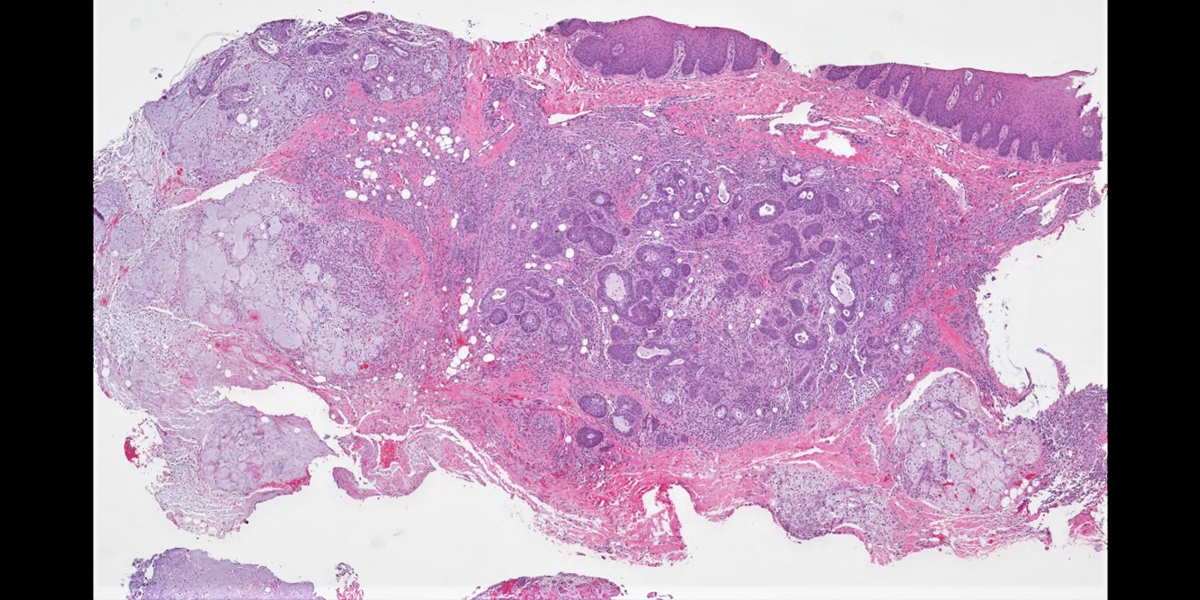
- Pseudoepitheliomatous hyperplasia of the overlying squamous mucosa, similar to that seen in granular cell tumor, may be present
- Preservation of lobular architecture. The maintenance of intact lobular architecture despite necrosis and inflammation is a key feature.
- Inflammation secondary to extravasation of mucin may include prominent acute and chronic inflammatory reaction and granulation tissue in or around the glands. This may mature to fibrosis, along with increased squamous metaplasia in an older lesion.
- Surface ulceration may or may not be present.
- Pertinent negatives: no evidence of infiltration, perineural invasion and lymphovascular invasion.
Squamous cell carcinoma (SCCa) and mucoepidermoid carcinoma (MEC) are the most commonly considered malignant lesions in the microscopic differential diagnosis. At low magnification, preservation of lobular architecture is a helpful histologic clue to NSM and excluding SCCa and MEC. Metaplastic squamous epithelial nests in the subepithelial connective tissue lead to consideration of a common diagnosis, such as squamous cell carcinoma. However, these squamous epithelial nests often show a bland cytologic appearance without dysplastic features. The absence of stromal invasion and the absence of disruption of lobular architecture are more reliable supporting factors for a diagnosis of NSM over SCCa or MEC. Regarding the latter, completely or partially necrotic salivary gland lobules intermixed with metaplastic lobules would be uncommon in MEC, particularly low grade MEC.
Once the diagnosis is established, treatment is symptomatic as the lesion is self limited. Complete healing is expected within 2 to 3 months. NSM does not usually recur, and if it is properly diagnosed preoperatively, surgical excision is not necessary. Lesions that fail to resolve should be reassessed.
Test Question Answer:
B. The palate is most commonly involved among the anatomic sites listed.
See more cases from PathologyOutlines.com




