A 38-year-old woman presents to the emergency department with chest pain for the past two days. The pain started gradually and is located in the center of her chest. It is slightly better when she sits up straight, and it is not affected by exertion or rest. The patient also reports feeling fatigued, achy, and feverish for the past few months. She takes no medications, and family history is non-contributory. The patient does not drink alcohol or smoke cigarettes. The patient’s temperature is 38.6°C (101.5°F), pulse is 104/min, respirations are 22/min, and blood pressure is 153/97 mmHg. She appears anxious and uncomfortable. Physical examination shows conjunctival pallor and bilateral pitting ankle edema, and a scratching extra heart sound between the apex and sternum is heard on auscultation. Laboratory studies show the following: Sodium 132 mEq/L; Potassium 4.2 mEq/L; Chloride 95 mEq/L; Hemoglobin 7.2 g/dL; Reticulocyte count 4.5%; Aspartate aminotransferase 20 U/L; Alanine aminotransferase 18 U/L; Bilirubin, Total 3.4; Bilirubin, Direct 0.3; Lactate dehydrogenase 368 U/L.
ECG shows the following:
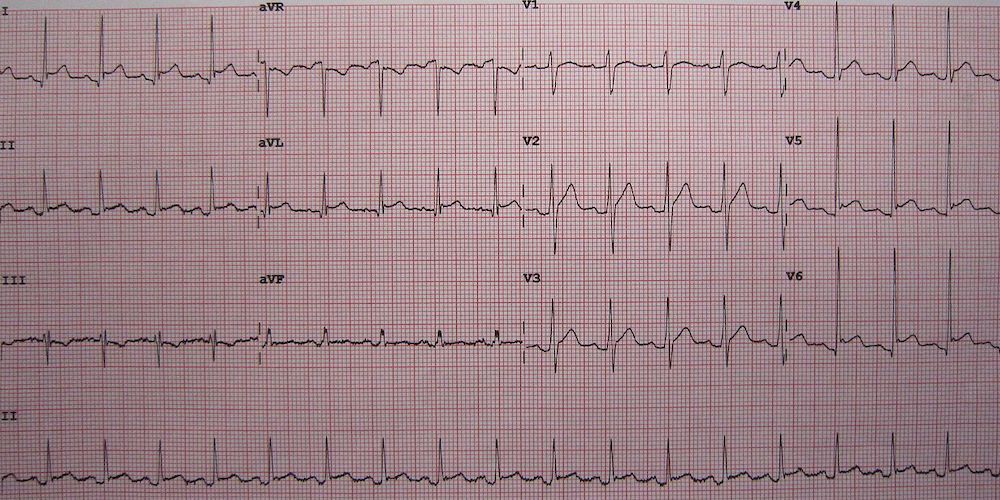
Reproduced from: Wikimedia Commons
Which of the following additional laboratory findings is most likely to be present in this patient’s condition?
A. Elevated fasting blood glucose
Incorrect: Although diabetes can cause renal damage over time, it would not explain this patient’s pericarditis or hemolytic anemia. Elevated blood sugar level is not associated with systemic lupus erythematosus (SLE).
B. Neutropenia
Incorrect: Although SLE may cause leukopenia and lymphopenia, a low neutrophil count (neutropenia) in isolation is not specifically associated with SLE.
C. Proteinuria
Correct: See Main Explanation.
D. Thrombocytosis
Incorrect: Hematologic effects of SLE include leukopenia, thrombocytopenia, and autoimmune hemolysis. SLE is not associated with increased hematologic cell counts, including platelets.
E. Uremia
Incorrect: Although increased serum urea nitrogen might result from a decreased glomerular filtration rate in the setting of lupus nephritis, elevated urea nitrogen itself is not associated with SLE.
Main Explanation:
This patient’s presentation is most consistent with systemic lupus erythematosus (SLE). The classic presentation of SLE is a reproductive-age woman with arthralgias, fevers, and rash; however, because autoantibodies can attack and damage any organ system in the body, there are a wide range of symptoms and laboratory findings that can suggest a diagnosis of SLE, as seen with this patient. This patient’s chest pain is most likely due to pericarditis, as evidenced by the constant nature, improvement with sitting up, and pericardial friction rub on auscultation. The laboratory studies demonstrate a hemolytic anemia as suggested by the reticulocytosis, elevated lactate dehydrogenase, and unconjugated (indirect) hyperbilirubinemia.
In general, the possible clinical manifestations of SLE include:
- Fever
- Hematologic
- Neuropsychiatric
- Mucocutaneous
- Serosal
- Musculoskeletal
- Renal
This patient exhibits 1) fever, 2) hematologic involvement, 3) serosal involvement (pericarditis), and likely 4) renal involvement, given her edema, which would be evidenced by proteinuria and a low serum protein level. Together, these findings make SLE the most likely diagnosis.
Major Takeaway:
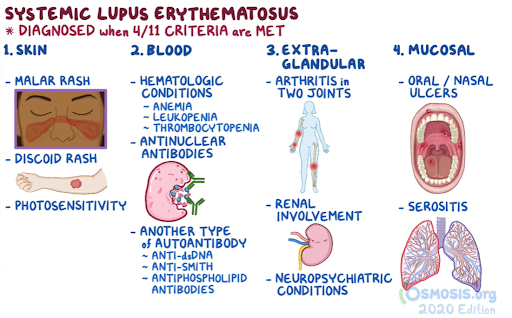
Systemic lupus erythematosus can be associated with the following: malar rash, discoid rash, photosensitivity, ulcers, serositis, renal disorders, neurologic disorders, arthritis, hematologic disorders, antinuclear antibodies, and other immunologic antibodies.
References:
Hahn, B. H. (2018). Systemic Lupus Erythematosus. In J. L. Jameson, A. S. Fauci, D. L. Kasper, S. L. Hauser, D. L. Longo, & J. Loscalzo (Eds.), Harrison’s Principles of Internal Medicine (20th ed.).





