


As an intern last year in internal medicine, I spent an inordinate amount of time performing a variety of non-medical tasks each day, collectively referred to by those in the medical community as “scut work.” While the definition of scut work varies among individual medical practitioners, it generally refers to any task that can be completed by an employee without a medical degree. In the past, this included many tasks that other hospital staff members could complete but were either unavailable or unable to do so. Think personally transporting patients to different areas of the hospital for scans and drawing blood for testing after hours.
With the rise of electronic medical records (EMRs) in recent years, the scope of tasks that comprise scut work has changed dramatically. In today’s modern setting, scut work includes, but is not limited to, the tedious processes of acquiring outside medical records; faxing medical records to other medical providers; spending hours on the phone with insurance companies to see if they cover various medications; filling out often irrelevant electronic documentation; scheduling outpatient follow-up appointments; and coordinating hospital discharges.
Of course, all of these tasks are crucial to ensuring that patients get the best quality of care and are set up for success once they leave the hospital. Someone has to complete them. But the crucial question is whether we should burden our medical residents, particularly our newest doctors (known as interns) with these tasks. (Residents of certain fields, like internal medicine, tend to be disproportionately burdened with scut.)
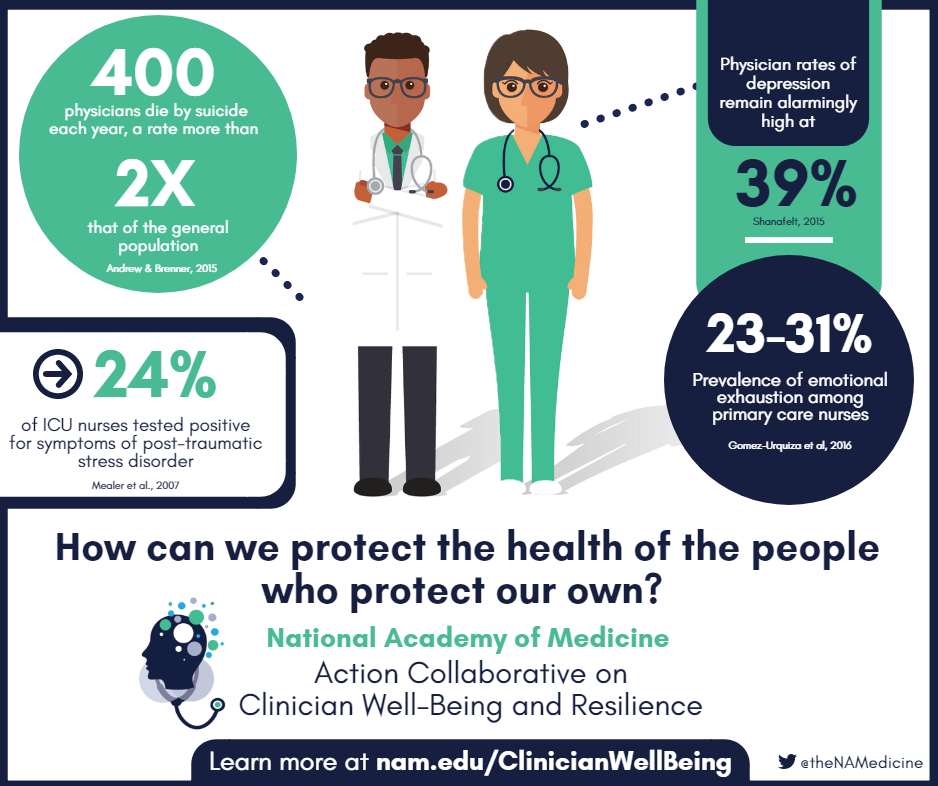
Scut work does not require four years of college and four years of medical school to complete and is widely viewed as non-educational for residents. If that was all there was to it, the phenomenon of scut work could potentially be tolerated. Most jobs in America require some degree of scut work. But the truth is there is ample reason to believe that scut work may be particularly dangerous in the field of medicine, for both patients and providers alike. Interns spend hours each day on EMRs, leaving less face-to-face time with their patients. And excessive scut work helps drive physician burnout, which can compromise both patient care and physician well-being.
On the other hand, the complex task of medically managing patients, the reason that most of us went to medical school in the first place, is emotionally and physically challenging, requiring an extraordinary amount of time, empathy, and resilience. As a stressed and overworked intern, I was preoccupied with ensuring that my patients were getting better. I certainly did not need the added stress of time-consuming scut work distracting me from my primary mission of caring for patients.
There are some preliminary signs that teaching hospitals are beginning to recognize the perils of dumping these tasks on their trainees. But the truth is that hospitals across the country have been slow to invest in the types of supportive services that would unburden their medical residents from these non-medical, often clerical tasks.
This is unfortunate. Decoupling scut work and the provision of medical care from the job responsibilities of residents could benefit hospitals in a variety of ways. Having more time to spend with patients could improve patient and resident satisfaction. Refocusing residents on their primary mission of learning to take care of patients would help combat physician burnout—and it could help improve patient outcomes.
As a second-year resident now in a different field, I have seen firsthand the benefits of reduced scut work. I am now able to focus the totality of my efforts on my training and my patients. Knowing that almost everything I do at work will be educational or directly benefit my patients, I come to work more energized and excited than I did at any point last year.
I only hope, for the sake of my co-residents in other fields, that other hospitals choose to follow this example in the near future.
Dr. Kunal Sindhu is a resident physician in New York City. You can follow him on Twitter @sindhu_kunal.
Dr. Sindhu is a 2018–2019 Doximity Author.






{kind=link}