

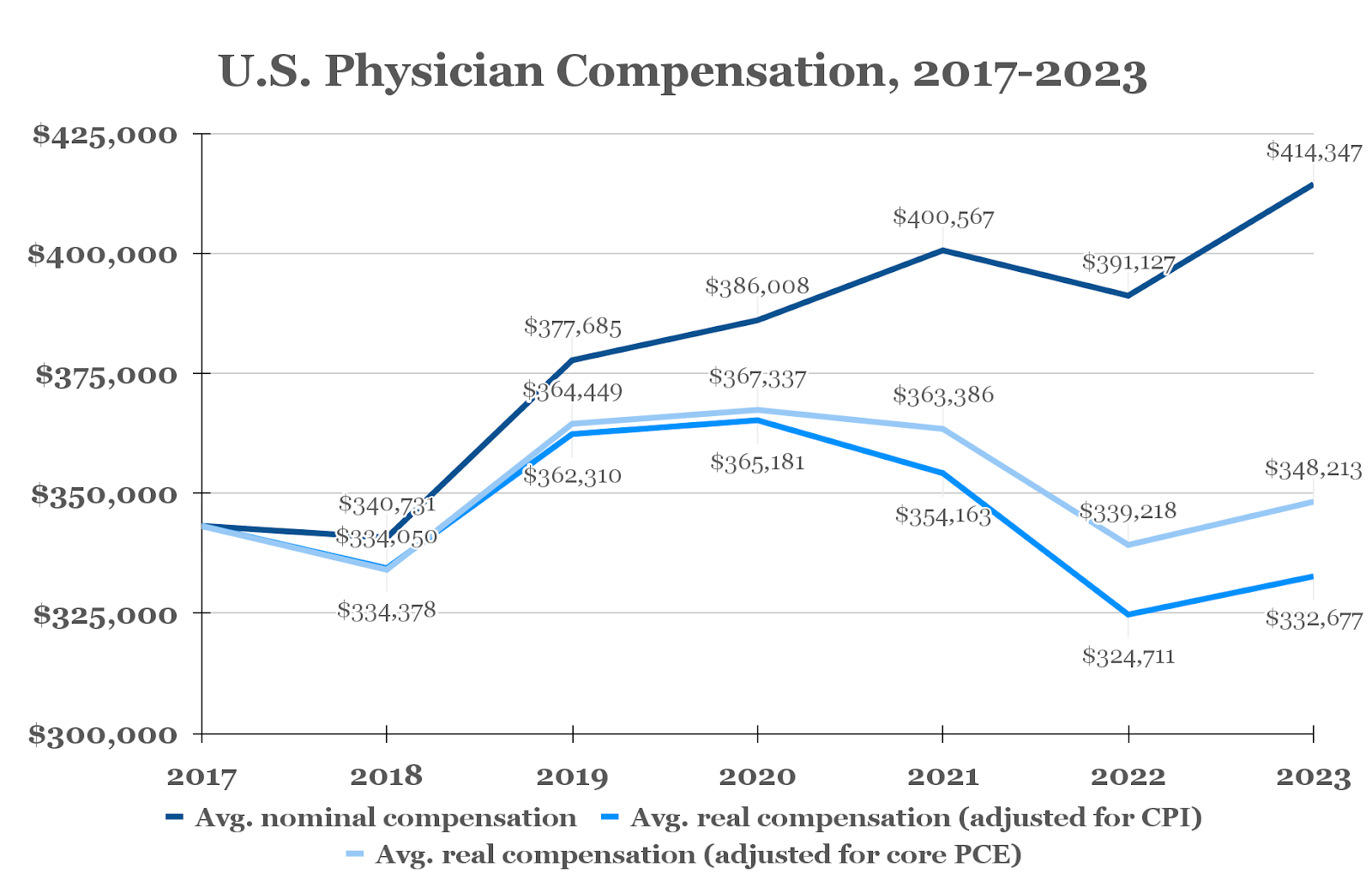
Average nominal physician pay reached $414,347 in 2023, up nearly 6% from the prior year, according to Doximity's 2024 Physician Compensation Report. After factoring in inflation, however, physicians’ real income and actual purchasing power has hardly budged over the past seven years, when Doximity first started reporting on physician compensation.
Real physician compensation was $332,677 on average in 2023, down 3.1% relative to 2017, after adjusting for inflation per the U.S. Bureau of Labor Statistics Consumer Price Index (CPI).
“The ‘golden days’ of medicine have passed,” Dan Fosselman, DO, sports medicine physician and chief medical officer of The Armory, told Doximity. “People feel that they are underappreciated for the work that they are doing.”
The Doximity compensation results reflect a pattern of stagnating, if not sinking, remuneration for an overworked labor force facing a rise in safety risks and shortages.
The situation has been especially punishing for Medicare physician pay, which, according to the American Medical Association, has fallen 26% since 2001 after adjusting for inflation.
A report by the Neiman Health Policy Institute found that Medicare conversion factor decreases and inflation from 2005 to 2021 would have lowered reimbursement even further were it not for a substantial increase in RVU volume — indicating that physicians now receive less pay despite producing more. In contrast, reimbursement for nonphysician practitioners increased 207% during the same period.
In addition to decreasing reimbursements, a wide range of factors may be contributing to the lack of growth in compensation, including declining physician ownership and insufficient opportunities to learn about or engage in contract negotiation and practice management.
High income is not a guarantee for financial security, and the reality is that physicians, who are often too busy to learn the optimal financial strategies, are not always the best financiers of their own money, according to Jeffrey Janis, MD of The Ohio State University Wexner Medical Center and Brett Janis, CFA, who cowrote a wealth and investment primer for physicians.
“In a way, we’ve been selectively trained to be altruistic; we donate our time and expertise, and though we want to be fairly compensated for it, pay is generally not the original, primary driver of why we entered medicine,” Dr. Janis told Doximity.
Pay by Specialty
Among 42 medical specialties studied, there was an overall decrease in CPI-adjusted real compensation for all but two from 2017 to 2023.
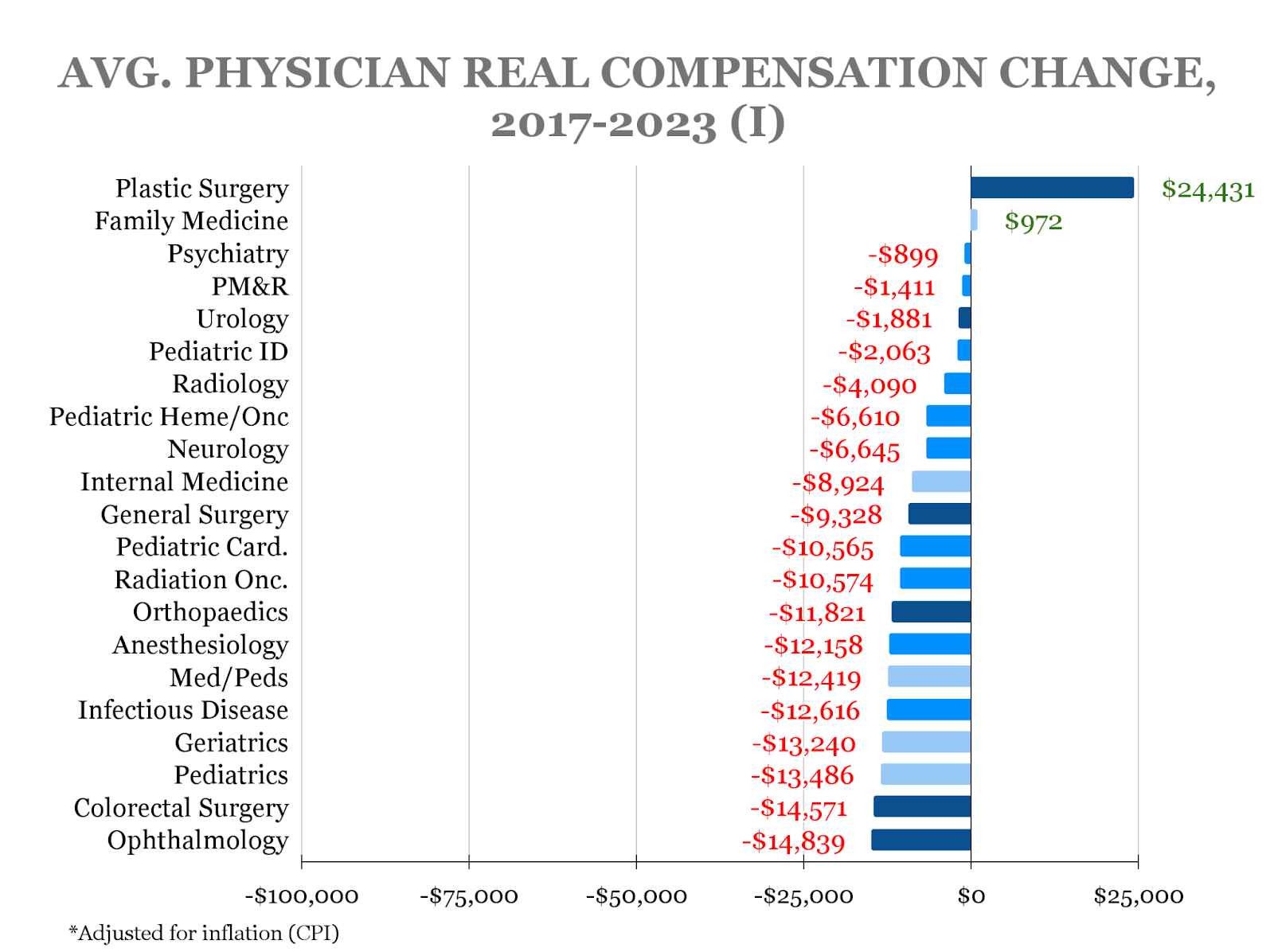
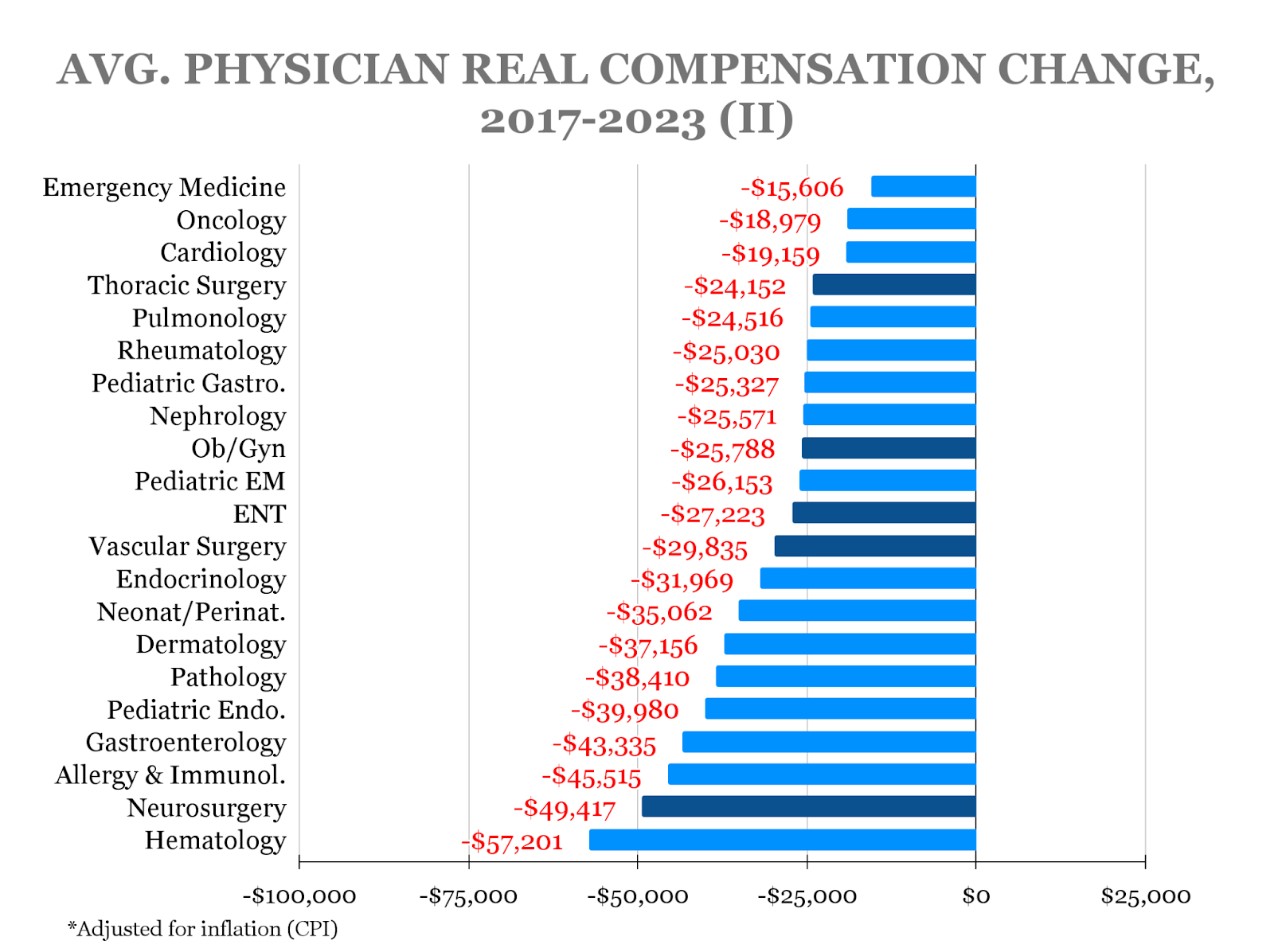
Hematology saw the largest decrease in total dollar amount (-$57,201), followed by neurosurgery (-$49,417) and allergy and immunology (-$45,515).
On average, pay for nonsurgical specialists declined by 7% (-$22,177), compared with 3.6% (-$16,766) for surgical specialties and 4% (-$9,419) for primary care. The drop in primary care real compensation was buffered in large part by a 0.4% ($972) increase for family medicine since 2017.
For most physicians, the rising cost of medical education further compounds the issue of decreasing pay, especially for specialties such as pediatrics that provide lower pay overall.
“As one of the lowest compensated specialties in medicine, pediatrics and pediatric subspecialties may not be viewed by medical students as viable options as they graduate medical school with large loans to pay back,” Sandy Chung, MD, immediate past president of the American Academy of Pediatrics, told Doximity. “This is complicated by the fact that CMS tends to undervalue nonprocedural care, which makes up most of pediatric care.”
Yet one specialty that has seen a jump in pay is plastic surgery, which had a real compensation of $497,643 in 2023, up 5.2% from $473,212 in 2017.
Unlike many other specialties, plastic surgery has a cosmetic component that follows an out-of-pocket cash pay practice model, which allows plastic surgeons to negotiate prices and reimbursement directly based on supply and demand, said Jordan Frey, MD, a plastic surgeon who offers financial advice under the moniker the Prudent Plastic Surgeon.
“A large proportion of plastic surgeons have some element of cosmetic surgery as part of their practice, and therefore those dollars are not subject to insurance-based pay reductions,” added Dr. Janis, a professor of plastic and reconstructive surgery.
“Then from the supply-demand curve … the ‘Zoom boom’ that occurred during the pandemic — where people were regularly looking at each others’ faces and necks, and at themselves — turned into an increased public interest in cosmetic surgery,” Dr. Janis continued. “And that’s still going on today.”
Location Matters
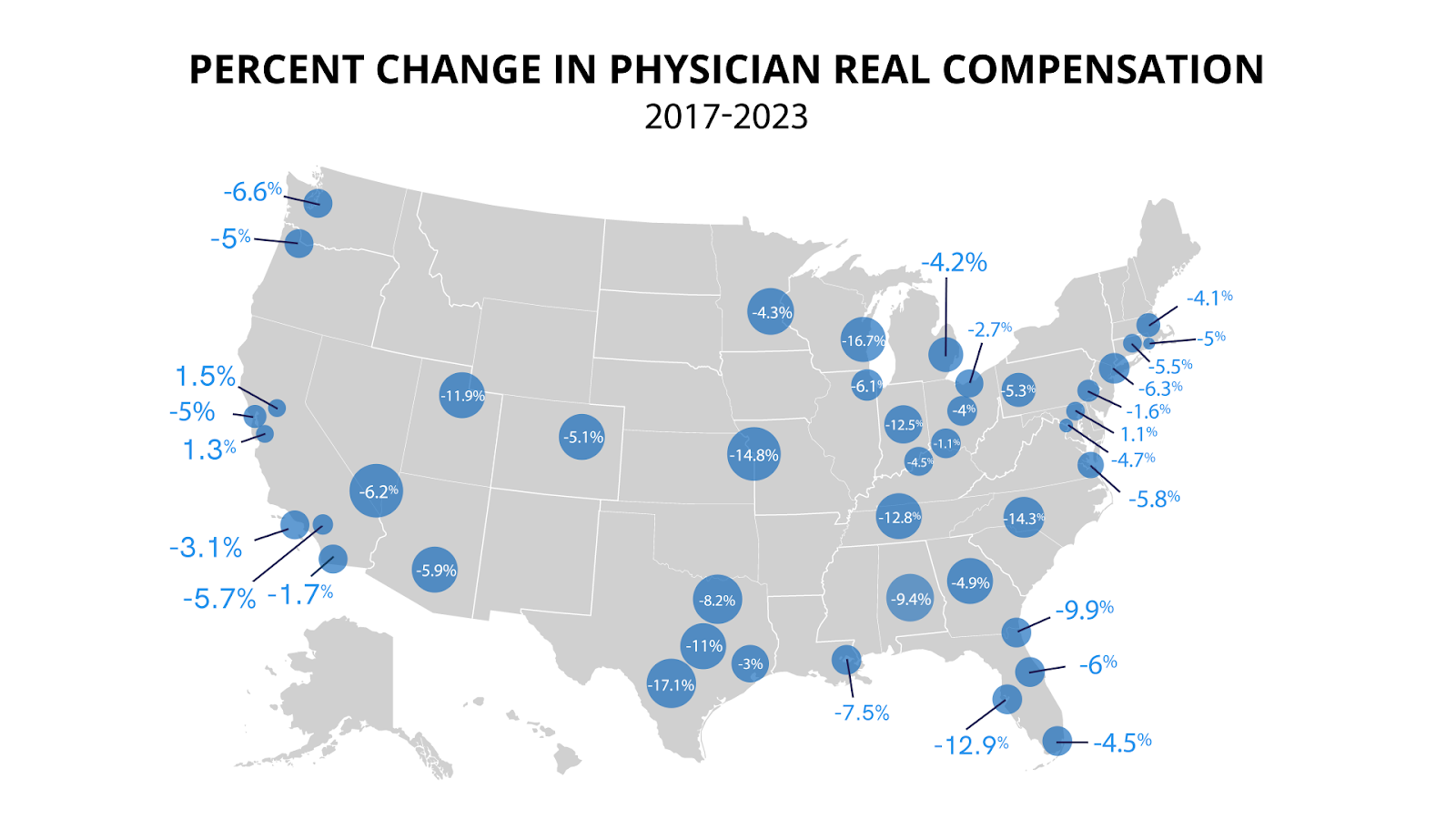
For physicians working in different metros, average real compensation decreased nearly across the board.
The three metros that saw positive growth from 2017 to 2023 were Sacramento ($5,215), San Jose ($4,771), and Baltimore ($3,376). (These changes reflect national CPI inflation adjustments that would differ if adjusted by local CPI.)
Average physician real compensation decreased in all other metros, including in some of the largest: Philadelphia (-$5,006), Houston (-$10,143), Los Angeles (-$11,433), Boston (-$12,917), Miami (-$16,119), Atlanta (-$17,232), Chicago (-$20,762), and New York (-$22,210).
Metros that saw the largest decrease were mainly those located in the South and Midwest: Milwaukee-Waukesha-West Allis (-$66,345); San Antonio-New Braunfels (-$61,576); Charlotte-Concord-Gastonia (-$57,377); Kansas City (-$55,060); Tampa-St. Petersburg-Clearwater (-$47,520); and Indianapolis-Carmel-Anderson (-$47,321).
In the case of one family medicine physician working at a residency program in the greater Milwaukee area, their compensation has not changed in over half a decade, despite being tasked with more responsibilities.
“During the pandemic, we were asked to do more and were not paid more,” they told Doximity under conditions of anonymity. “I have not received a raise since starting my job over five years ago.”
Not only do many physicians say that work-related raises are uncommon, but basic cost-of-living adjustments that match inflation are exceedingly rare as well.
Over the past two years, Dr. Janis’ university practice plan rewarded his increase in work with a 2% raise each year, amid a surge in inflation that peaked at over 9%.
“While an increase is definitely appreciated,” Dr. Janis said, “in real dollars, it doesn’t keep pace with inflation, resulting in a net loss of purchasing power despite higher productivity requirements.”
‘On Your Own Terms’
To a large extent, physicians believe that they are underpaid. Only 40% of the physicians who were surveyed are satisfied with their current pay, and 62% believe their compensation does not sufficiently reflect the level of expertise and effort required for their role.
Yet most physicians (63%) have either not requested higher pay or been unsuccessful in their attempts to do so. Instead of seeking higher pay, the community seems to be in favor of more flexible work conditions: 75% of physicians surveyed have accepted, or are willing to accept, lower pay to achieve more autonomy or work-life balance.
“Medicine teaches us to always put patients first,” the Milwaukee-area family physician told Doximity under conditions of anonymity. “So we spend our energy and time advocating for patients and probably don’t spend enough energy and time advocating for ourselves.”
The other challenge for physicians is that negotiation can be taxing to wade through, often demanding more work than is worth the small return it may not even bring.
“There are some institutions and organizations that don’t afford much room for negotiation with individual physicians,” Dr. Janis said. “Oftentimes, compensation is tied to national benchmarks, which don’t always take the whole picture into account.”
What’s more, decreasing reimbursements have led many physicians to transition out of their independent practices and either move to another state with a lower cost of living or seek work under a more stable employer-based model.
In light of surging costs and a gridlock in pay, neurologist Rikki Racela, MD, felt compelled to sell his private practice to a nearby hospital.
“Working under a productivity model has been more pay for me as I no longer have to deal with insurance denials or patients not having insurance,” Dr. Racela, a regular contributor to the finance blog White Coat Investor, told Doximity. “But I have lost autonomy, where my boss could tell me to work harder and put me on call more often, and I can’t do anything about it.”
Dr. Racela’s experience has motivated him to better manage his finances in order to build more leverage moving forward — an approach that he suggests other physicians consider.
“Physicians can run into financial issues of overspending and living beyond their means because a doctor’s salary can no longer maintain a typical ‘doctor lifestyle,’ leading to burnout,” he said. “But if your personal finances are in order, you are in a position of strength to negotiate for higher salaries or maybe start a private practice without worrying about needing some immediate cash flow.”
Dr. Frey agreed on the importance of personal finance and encouraged physicians to start with basic financial hygiene, such as saving 20% of gross income; investing in broadly diversified, low-cost index funds; paying off debt; and creating alternative sources of income.
“Build good habits that will lead to financial freedom — the concept that you can work and practice medicine because you want to and on your own terms, not because you have to,” Dr. Frey said. “The more doctors who become financially free, the more it will help physicians take back control and improve health care overall.”
Still, he emphasized that decreasing compensation is ultimately “a system-wide issue and will not be solved rapidly.”
Experts in physician finance suggest that broad, long-lasting changes to pay and reimbursement will require ongoing advocacy from the collective physician body.
“We need to take ownership of the duty of our profession,” Dr. Fosselman said. “The duty of our profession is to provide great care for patients. Great care requires effective systems in a clinical and administrative context.”
The policy and institutional changes needed to improve the current pay and care structure “require persistent energy and effort that will come at a personal cost,” he added. “Too many of us are trading the opportunity of improving health care delivery for short-term security in the form of higher pay or benefits. The system won’t fix itself.”
Image by eamesBot / Shutterstock





