
Nonpromotable tasks are particularly common among women in medicine, with over three-fourths spending more than 10% of their work time on these tasks, according to a Doximity poll of 649 women conducted in August 2023.
Physicians are often involved in nonpromotable tasks — important but general work that does not lead directly to promotions, such as serving on committees, planning department events, providing feedback, or certain administrative tasks.
Studies have shown that women receive more requests for nonpromotable tasks and spend more time on them, often resulting in a negative impact on their career.
“Research has suggested that women are more likely to volunteer for nonpromotable tasks than men,” Michelle Izmaylov, MD, assistant professor of clinical medicine at Vanderbilt University School of Medicine, wrote in an Op-Med. “These are tasks that are not likely to impact the performance assessments that determine whether an individual would be considered for a promotion.”
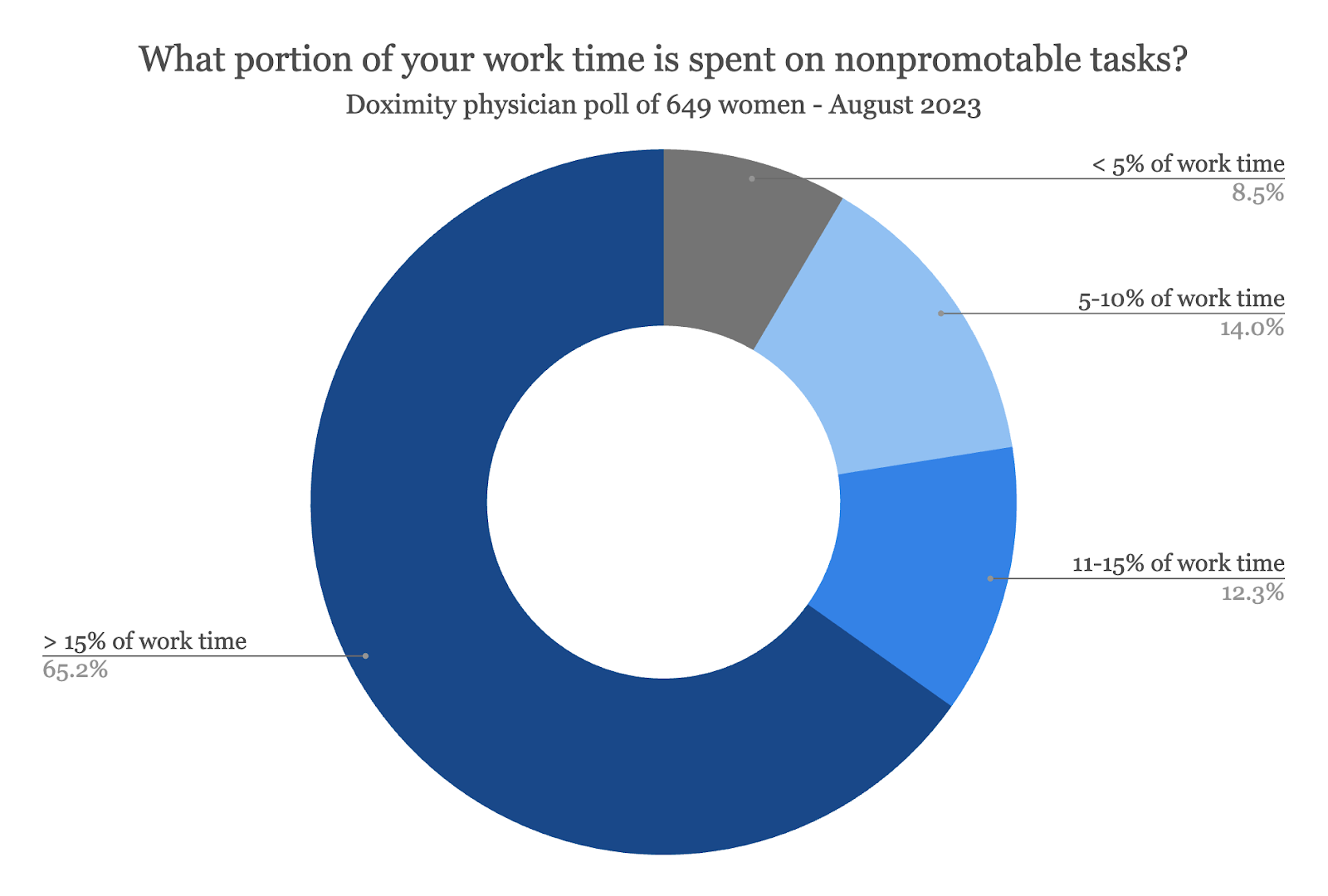
Indeed, the poll results show that most women (65%) spend at least 15% of their work day on nonpromotable tasks. In comparison, 12% of women say that they spend 11%-15% of their time on these tasks; 14% of women spend 5%-10% of their time; and only 9% spend less than 5% of their time.
“If you want to do a good job on notes, follow up, referrals — you need to spend more than 15% of your time [on nonpromotable tasks],” said geriatrician Kimberly Miller, DO.
Regardless of the type of specialty, most women spend more than 15% of their work time on nonpromotable tasks: 64% of primary care physicians, 65% of surgeons, and 66% of nonsurgical specialists.
Nonpromotable tasks seem to be most prevalent among women in the middle of their career. At least 70% of midcareer physicians spend more than 15% of their time on nonpromotable tasks, compared with 63% of early career physicians and 61% of late-career physicians.
Women physicians are often placed in a double-bind, as some of this nonpromotable work can include serving as mentors and on hiring committees or contributing to diversity, equity, and inclusion efforts. Saying “no” to such nonpromotable work can compound the problem of inequality and lack of representation.
“Being 'volun-told' for tasks and having it be promotable can be two different, though interrelated challenges,” said Kimberly Clare, MD, a pediatrician and division manager of a multispecialty group.
Earlier in her career, Dr. Clare would spend a considerable portion of her day on uncredited administrative work — such as updating EMR templates and running quality reports — with a slight adjustment to her compensation to account for the work. When her office merged with a multispecialty group after 20 years of practice, it removed the adjustment to her pay, and so she reduced the amount of time she spends on those tasks to an hour per day.
“My work on quality generates over $250,000 per year for my division but I don't get direct credit for any of it,” she said. “If I decided to stop doing this other stuff, it would fall onto my overtaxed administrator who struggles with her own sheaf of nonpromotable work.”
Some physicians have suggested that hospitals and practices could consider exploring ways to compensate for nonpromotable tasks rather than reduce the amount of time they spend on them.
“Perhaps the goal would not be to eliminate these activities, but to make them ‘count’ and carve out time for them,” said Melissa Schiffman, MD, an internist in Pennsylvania.
“We get told that these committees, etc. count toward ‘citizenship’ points, but it's like your attendance/class participation grade at school,” added Dr. Clare. “It counts, but not enough to raise your grade. Until our core values are different, until the game is different, nothing will change.”
Vineet Arora, MD, Dean for Medical Education at the University of Chicago Pritzker School of Medicine, advised women physicians to “always think about what is in it for you and what is in it for the organization. For very junior people, it may be that the calculus favors being a good citizen to build [your] internal reputation so [you] can get larger opportunities. For example, one rarely rises to the level of being a senior program leader in education by not participating in such tasks and developing a reputation as a good citizen.”
On the other hand, Dr. Arora acknowledged that good citizenship and service to nonpromotable work are "often not seen as valuable or externally facing for promotion [in a health system], which leverages national reputation and also values things like publications.”
“It’s probably a good idea to keep track of such tasks like committee service and make sure there is some reward for participating that counters the issue of ‘nonpromotable,’” Dr. Arora added. “The idea that something is ‘nonpromotable' but has institutional value of some sort is in fact part of the problem and should be addressed with system-level solutions.”
Dr. Izmaylov echoed the approach, recommending physicians who are engaged in nonpromotable work to let their supervisor know how they are applying their skills to that work and how they might be able to apply those skills to other, more valued projects as well.
“For example, many academic medical centers are interested in clinical performance and professional contributions,” Dr. Izmaylov said. “As you volunteer for tasks at your organization, consider what work is more likely to contribute to promotion for you. There may be a way to turn your project into a promotion.”
Image: Masanyanka / gettyimages





