
A digital rectal exam (DRE) is a vital component of the male physical exam in which a gloved, lubricated finger is placed gently within the rectum to examine the outer, accessible surface of the prostate and gain valuable information about its health. An annual DRE is highly recommended after age 40. Although not a pleasant examination, it is brief and not painful. Urologists do not relish performing a DRE any more than a patient desires receiving one, but it provides essential information that cannot be derived by any other means. If the prostate has an abnormal consistency, a hardness, lump, bump, or simply feels uneven and asymmetrical, it may be a sign of prostate cancer, the most common cancer in men and one that causes no symptoms in its earliest stages. Prostate cancer most commonly originates in the peripheral zone of the prostate, the region that is accessible via DRE.
“The only circumstances in which a male patient does not get a DRE is if he has no rectum, the physician has no finger, or the patient is having an acute cardiac event.”
Dr. Ganesh Pallauttu (Chairman of Urology, University of Michigan), paraphrased from a recent lecture.
DRE in conjunction with the prostate-specific antigen (PSA) blood test are the best tools to screen for prostate cancer. Some patients have told me that their PCPs informed them that a PSA test can replace the DRE. That is blatant misinformation. The truth of the matter is that the two tests are complementary — each providing unique information — and it is entirely possible to have prostate cancer with a normal PSA, the cancer presenting only with an abnormal DRE. Detection rates for prostate cancer are highest when using both tests, followed by PSA alone, followed by DRE alone. The pathological features of prostate cancers detected on an abnormal DRE are generally less favorable than those of cancers detected by a PSA elevation. In other words, if the cancer is palpable, there is more concern than if it cannot be felt, as it is often at a more advanced stage.
Some aggressive and poorly differentiated prostate tumors are notorious for being so undifferentiated that they do not elaborate much PSA, particularly neuroendocrine tumors that are primarily diagnosed by an abnormality on DRE.
These are high-tech times, and we have all sorts of fancy and sophisticated imaging tests to evaluate the prostate, e.g., multiparametric MRI, but the good old DRE remains a vital part of the physical exam of a male patient and should never be marginalized or forsaken. In addition to providing valuable information on prostate size, symmetry, and palpable irregularities, it also offers insights about anal/rectal tone, the presence of rectal masses, and the tonicity of the pelvic floor muscles, and allows for testing for occult blood. The price of DRE is right while the price of not doing one can be costly if a delayed diagnosis of prostate cancer is the outcome. Many patients expect a DRE as part of a physical exam, and many will question the thoroughness of an exam that does not include one.
Within the last month, I picked up a rectal cancer on DRE done for purposes of examining the prostate. The prostate felt fine, but the rectum overlying the prostate felt rough and irregular, and the diagnosis was confirmed upon referral to the colorectal surgeon.
DRE is clearly dirty business for the physician wielding the digit, certainly much less refined than examining a patient with a stethoscope. It is also momentarily uncomfortable for the patient. Nonetheless, it is necessary business. If a physician is apprehensive about doing a DRE or they question their digital diagnostic skill and acumen, simply referring the patient to a urology colleague is in order. It is our pleasure.
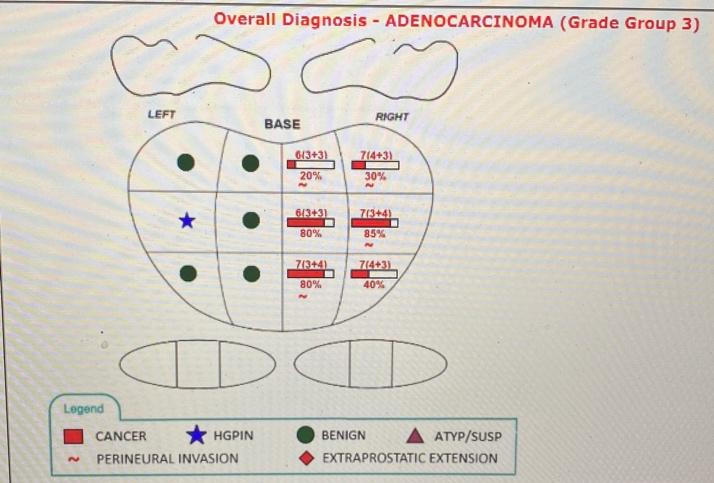
Case Study: A 50-something-year-old male was referred for evaluation of urinary frequency. His DRE revealed asymmetry, with the right side of the prostate firmer than the left, and he had a PSA of 2.2. He underwent prostate biopsy that showed an aggressive Gleason 7 (4+3) cancer that was managed with a robotic-assisted laparoscopic prostatectomy. The urinary frequency had nothing to do with the prostate cancer, since most early prostate cancers cause no symptoms, hence the need for screening DRE and PSA. Had this man not had the DRE and only had the PSA, this cancer would have been missed and the potential for curative intervention lost.
Bottom Line: Prostate cancer is the most common malignancy in men (aside from skin cancer) and in its earliest phases is most often asymptomatic, thus the need for screening with DRE and PSA. Prostate cancers are occasionally diagnosed because of an abnormal DRE, even in the face of a normal or low PSA. The DRE is a vital part of the male physical exam that provides valuable information and should not be forsaken.
Dr. Siegel is a New York metro area urologist who writes a weekly health and wellness blog and is the author of several health-related books, including “Prostate Cancer 20/20: A Practical Guide to Understanding Management Options for Patients and Their Families.”
Illustration by Jennifer Bogartz and April Brust





