
During the 2021 ACG Postgraduate Course, Dr. Aasma Shaukat provided an update on appropriate follow up of patients after a screening colonoscopy. The 2020 recommendations from the U.S. Multi-Society Task Force on Colorectal Cancer provided some significant changes to previous practice. The follow up is based on the number and type of polyps found during the index colonoscopy.
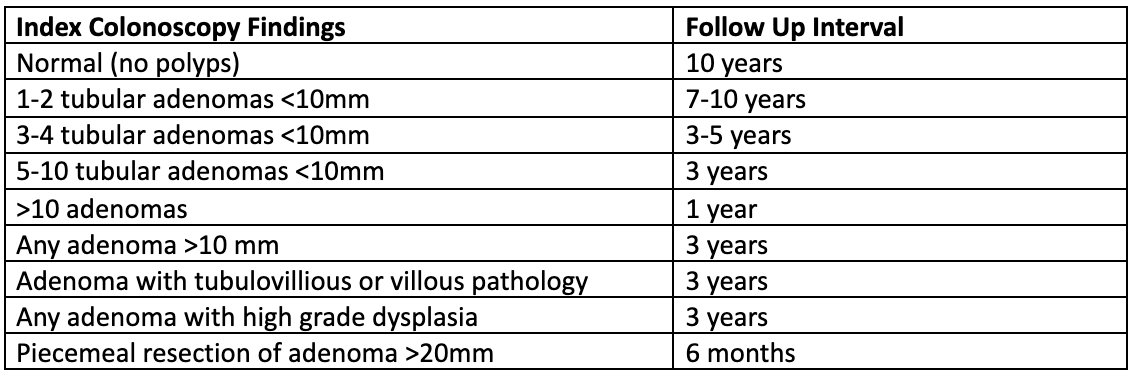
For colonoscopy to be safe and cost effective, proper attention must be paid to follow up intervals. The task force gave ranges rather than definitive intervals for two of their recommendations, but Dr. Shaukat emphasized that with a high-quality initial colonoscopy including adequate preparation and careful examination, the longer intervals in the ranges are very reasonable. Since the number of adenomas markedly changes follow up intervals, it is important for the endoscopist to attempt to find all polyps, including very small ones, during the index exam. The biggest change is that patients with one or two small adenomas can be managed similarly to those with a normal colonoscopy. Some of the other intervals are changed less.
The task force also nicely addressed what interval should follow future surveillance exams. Basically, if the index colonoscopy had four or fewer small adenomas, the interval between the second and third colonoscopy should be based on what is found during that second colonoscopy. For example, four polyps on the first colonoscopy and two or fewer on the second colonoscopy would push the patient to 10-year follow up after the second colonoscopy.
In addition, patients with up to 20 hyperplastic polyps can be managed like a normal exam with 10-year follow up. Polyps with serrated histology have a slightly more aggressive interval, but still should be no more frequent than three years unless the lesions are large and have been removed in a piecemeal fashion. Finally, the recommendation to begin screening at age 45 continues.
To put this in perspective, if an average risk individual has one or two small adenomas at age 45, formerly they would have a colonoscopy every five years. Now if they have no more than one or two adenomas on any of their exams, they can have a colonoscopy every 10 years. This avoids exposing them to the inconvenience, expense, and the small risk of three colonoscopies in their lifetime with minimal to no increase in cancer risk. Gastroenterologists, primary care providers and patients should know about and follow these updated guidelines.
Dr. DeVault has no conflicts of interest to report.
Image by Naeblys / Shutterstock





