A 26-year-old man presents to your osteopathic manipulation clinic due to difficulty turning his head for the past six days. He spent most of last week studying for his school exams. He has no headaches, neck pain, photophobia, phonophobia, or fever. He has attention deficit hyperactivity disorder which is well controlled with atomoxetine 80 mg daily. His temperature is 37.8 ºC (100.0 ºF), pulse is 66/min, respirations are 12/min, blood pressure is 115/70 mmHg. Osteopathic structural examination shows significantly restricted rotation to the left at C4. Translation at C4 is easier from right to left. Upon flexing his neck, rotation is much easier at C4. There is no significant tenderness to palpation or tissue texture change. Manipulation of the entire cervical spine does not elicit any pain. How would you treat his cervical spine somatic dysfunction with osteopathic manipulation?
A. Perform HVLA by flexing at C4, sidebending left and rotating left
Incorrect: While the sidebending and rotation are correct here, his full barrier also includes extension. In order to set up for HVLA, you need to engage his barrier via extension, left sidebending and left rotation.
B. Perform HVLA by extending at C4, sidebending right and rotating right
Incorrect: While the extension is correct here, his full barrier would involve sidebending left and rotating left. In order to set up for HVLA, you need to engage his barrier via extension, left sidebending and left rotation.
C. Perform muscle energy by flexing at C4, sidebending right and rotating right
Incorrect: This represents his somatic dysfunction (freedom of motion). In order to treat with muscle energy, you need to engage his barrier by moving his C4 directly opposite of its somatic dysfunction.
D. Perform muscle energy by extending at C4, sidebending left and rotating left
Correct: See Main Explanation.
E. Avoid HVLA due to concerns for meningitis
Incorrect: Osteopathic manipulation of the cervical spine should be avoided in patients with signs and symptoms concerning for meningitis. In this patient, his lack of symptoms, normal vital signs and supple neck all point away from meningitis.
Main Explanation
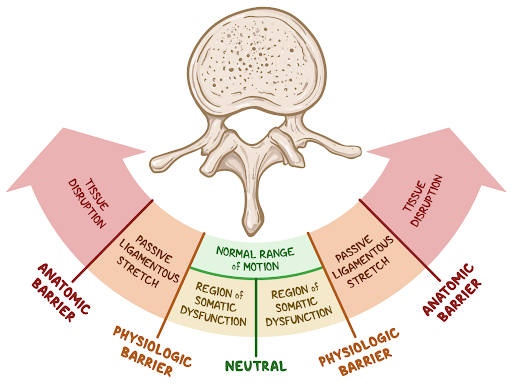
Diagnosis of cervical spine (C2-C7) somatic dysfunctions involves assessing flexion/extension, rotation (side of prominent articular pillars) and sidebending (opposite of ease of translation). The cervical vertebrae almost always sidebend and rotate to the same side, behaving similarly to type II Fryette mechanics, so you do not need both rotational and sidebending findings to make the correct diagnosis.
Treatment with muscle energy or HVLA of the cervical spine is similar to other areas of the body. Position the patient into their barrier by moving exactly opposite of their somatic dysfunction. For HVLA, you perform a low amplitude thrust after engaging their barrier. For muscle energy, you instruct the patient to move toward neutral (i.e. in the direction of their somatic dysfunction) as you gently engage their barrier. When performing an HVLA thrust of a flexed dysfunction, always remember to only extend at the level of the specific vertebra and not the entire cervical spine up to that level.
Major Takeaway
In order to treat cervical spine somatic dysfunctions with muscle energy or HVLA, place the patient exactly opposite of their somatic dysfunction to engage their physiologic barrier. For muscle energy, instruct the patent to return to neutral by moving in the direction of their somatic dysfunction.





