


One of my first coaching experiences occurred when I was on my swim team in middle school. I was a subpar swimmer, especially when I compared myself to the peers in my age group. However, my coach at that time identified potential in me. At the end of practice she approached me and said she thought I could do better and quickly identified focus areas. She believed I could qualify for one of the state swim meets, which would require me to shave a full two seconds off of my time.
So I practiced. I felt motivated to pick up running and other strengthening exercises, ask her if I was correcting my form, and review my stroke. After each meet when my times started to drop by half a second, she encouraged me and continued to provide strategies for improvement. I eventually made the time and was able qualify for our state swim meet.
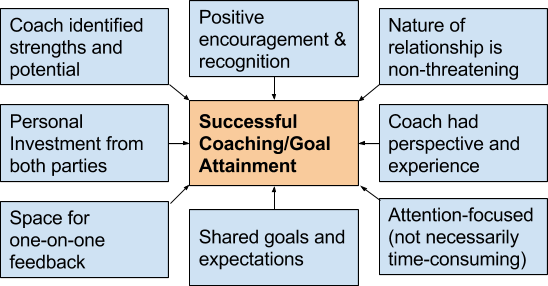
I now realize this coaching experience was defined by the following themes:
In my medical school clinical rotations, the way of teaching is often seems limited to traditional roles of “teacher” and “student”. Main interactions are centered around lecturing about topics, asking “pimping” questions, and evaluating students performance in typically brief objective interactions involving presentation of patients and formulation of diagnostic/treatment plans. Undoubtedly, this method has produced successful, careful, and diligent physicians for many decades. However, as I constantly hear technology change, scientific innovation transform, and the way we interact with the world evolve, it is surprising medical education has yet to make smaller strides.
The idea of coaching in medical training is not novel. Dr. Atul Gawande has written about its usefulness in the operating room, the American Medical Association has written a guide for its application in medical advising, and many of the key tenets of coaching are practiced in mentor-mentee relationships. The value of coaching has been applied to resident education, but appear less present in medical student clinical education. Coaching can improve clinical medical education by providing a supportive learning environment to improve student competencies required on rotations and ultimately sustain long-term skill building and clinical knowledge.
Most recently, when I was speaking with Dr. Thomas Varghese, associate professor in cardiothoracic surgery at University of Utah, I admired his approach to medical education. For third year medical students on core clinical clerkships, he discusses his expectations for knowledge and skills to the medical student in a safe, one-on-one setting at the scrub sink prior to the start of his cases. He describes this as a setting a speed limit, in which the students can choose to go above or below the expectations. The standards are adjustable with more experience and knowledge, especially once students are at the acting intern level. Following clinical interactions, he then sets aside time for private feedback.
There are a few reasons why I like this method. It does not put the medical student unexpectedly on the spot. It provides a non-threatening space for medical student self-assessment with a “coach”. There is an early discussion of expectations prior to the clinical evaluation. These factors increase medical student investment and clinical engagement. Although negative experiences from traditional approaches can also motivate medical students, they can lead to professional burnout and negatively impact the educational experience.
Clinical medical education does not need to be unnecessarily difficult. In the wealth of evidence-based medicine, resources for medical knowledge of disease processes, and an increasing number of specialties and subspecialties, it is daunting for medical students rotating for only a few weeks at a time on a new service to know where to start. Providing a roadmap and supplementing with coaching may transfer to producing competent clinicians who can also pave a brighter future in medicine.

Shree Agrawal is a fourth year medical student at Case Western Reserve University, where she also completed her bachelors of science degree in biology. Currently, she is completing a clinical research fellowship in genitourinary reconstruction at the Glickman Urological and Kidney Institute at Cleveland Clinic and serving as the Chair of the AWS National Medical Student Committee. Shree is passionate about research surrounding patient decision-making and medical education. In her free time, she enjoys blogging, practicing yoga, and boxing. Twitter: @ShreeAgrawal21
No conflicts of interest to disclose.





