We were in the resident work room when a senior resident announced he was heading to Palm Springs for the weekend.
“It’s gonna be like 100 degrees. Hey, Njeri, can I, like, borrow your skin this weekend?” He turned to me and said, laughing.
I looked up from my computer. “Excuse me?” I was sure I had misheard.
“Your skin, I wish I could borrow your skin.”
I was quietly processing his words. “My sk-kin?” I dragged out the word, just to be sure we were on the same page.
He went on to explain what I had feared was his reasoning. “I just burn so easily,” he said, as he lifted his hands to his face, twisting them slightly. He casually adjusted his glasses, then continued charting.
My co-intern was seated across the room. I looked back at him appalled and caught his gaze. He widened his eyes, shifted them from me to the senior resident and then back to me before raising his phone in the air. He wiggled it to signal that I should check mine. I opened his text: “Is he for real right now? I am so sorry.”
I swallowed the discomfort that was building in the back of my throat before responding. “You don’t think Black people … can get sun damage?”
At first, confusion sat doe-eyed on his face. It quickly morphed into a defensive wrinkled brow. “No, ‘cause … well, no. I mean, how?”
“Melanin is protective, but the effects of sun damage can still cause skin cancer. It’s usually found much later in Black people 'cause we don’t think to look for it. Also, we all feel the sun’s heat equally.”
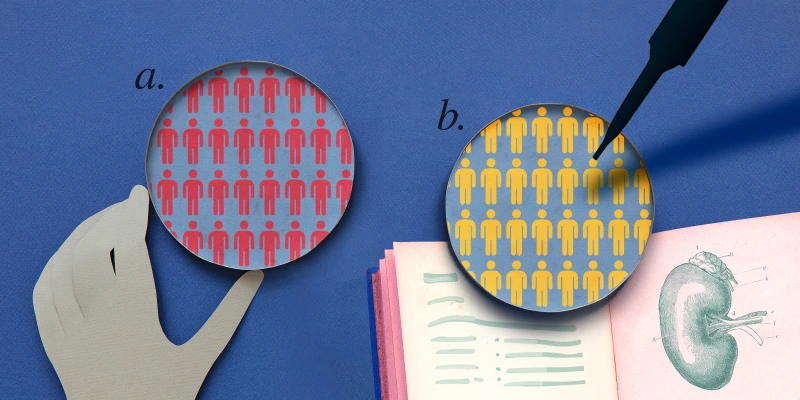
Although Black people are far less likely to develop melanoma than non-Hispanic white people due to the protection of melanin, Black people who develop skin cancer have a much lower five-year survival rate. The CDC found that, from 2011-2015, the five-year survival rate in the U.S. for Black patients was 66%, compared with 90% for non-Hispanic white patients. Contrary to popular belief, all persons are susceptible to sun damage, and sunscreen should be advised as primary prevention in conjunction with a yearly full-body skin exam.
I recognize that the fault in my former colleague’s reasoning may lie in the hands of medical education, due to its limited representation of pathology on Black skin. Skin of color darkens in the sun, and one can observe this change a few hours after sun exposure when comparing areas covered by clothing. While it may not peel and redden, the sun’s effects are quite noticeable. It is dehumanizing to think that one’s skin, no matter its shade, can sustain the discomfort of 100-degree weather. Do I not feel the same pain as him?
This experience opened my eyes to the critical role of medical education and training in preparing clinicians for the evolving demographics of the U.S. population. Several key lessons I have learned since then include the following:
First, it is imperative to unlearn any preconceived perceptions of varying pain tolerance among racial groups. A study in 2016 showed that some medical students and residents still think Black patients feel less pain than white patients. While the red and purple hues of bruises, cuts, and welts juxtaposed against white skin appear more jarring, patients with skin of color feel the same pain with less jarring changes to their skin tones.
Second, I took it upon myself to learn how common diseases present on skin of color. Unfortunately, one cannot go back to basic sciences in medical school and relearn the basics of dermatology, so I was proactive in teaching myself. As an internal medicine resident, there are certain diseases I should be able to recognize, or at least suspect and treat, and know when to refer out. I started by using a resource called Visual Diagnosis by following their informative social media page. I learned how chicken pox, cellulitis, psoriasis, urticaria, tinea versicolor, vitiligo, squamous cell carcinoma, and acral melanoma present on skin of color. I also learned, after a whole year of attributing the dry, flaky skin around my neck to N95 contact dermatitis, that I, in fact, had eczema. I had never seen it on a Black person before, so I couldn’t recognize it even on my own body.
While it was painful to be viewed as someone with skin that could be used as a shield from the sun, it was more painful to realize my former colleague, nearing the end of his training, was unaware sun damage occurs in skin of color — and may have potentially overlooked relevant concerns in this patient population.
We all feel the sun’s heat.
How can medical education and training better adapt to evolving patient demographics? Share your ideas in the comment section.
Dr. Kuria is an internal medicine resident physician in Loma Linda, CA who’s passionate about preventing heart disease. She enjoys museums, traveling, and trying new vegetarian recipes. She tweets at @kuriascase. Dr. Kuria is a 2022-2023 Doximity Op-Med Fellow.
Image by Natalie Magee / EyeEm / GettyImages