Amid a growing call for better working conditions in health care, a recent Doximity poll showed that 64% of clinicians who responded are willing to join a union.
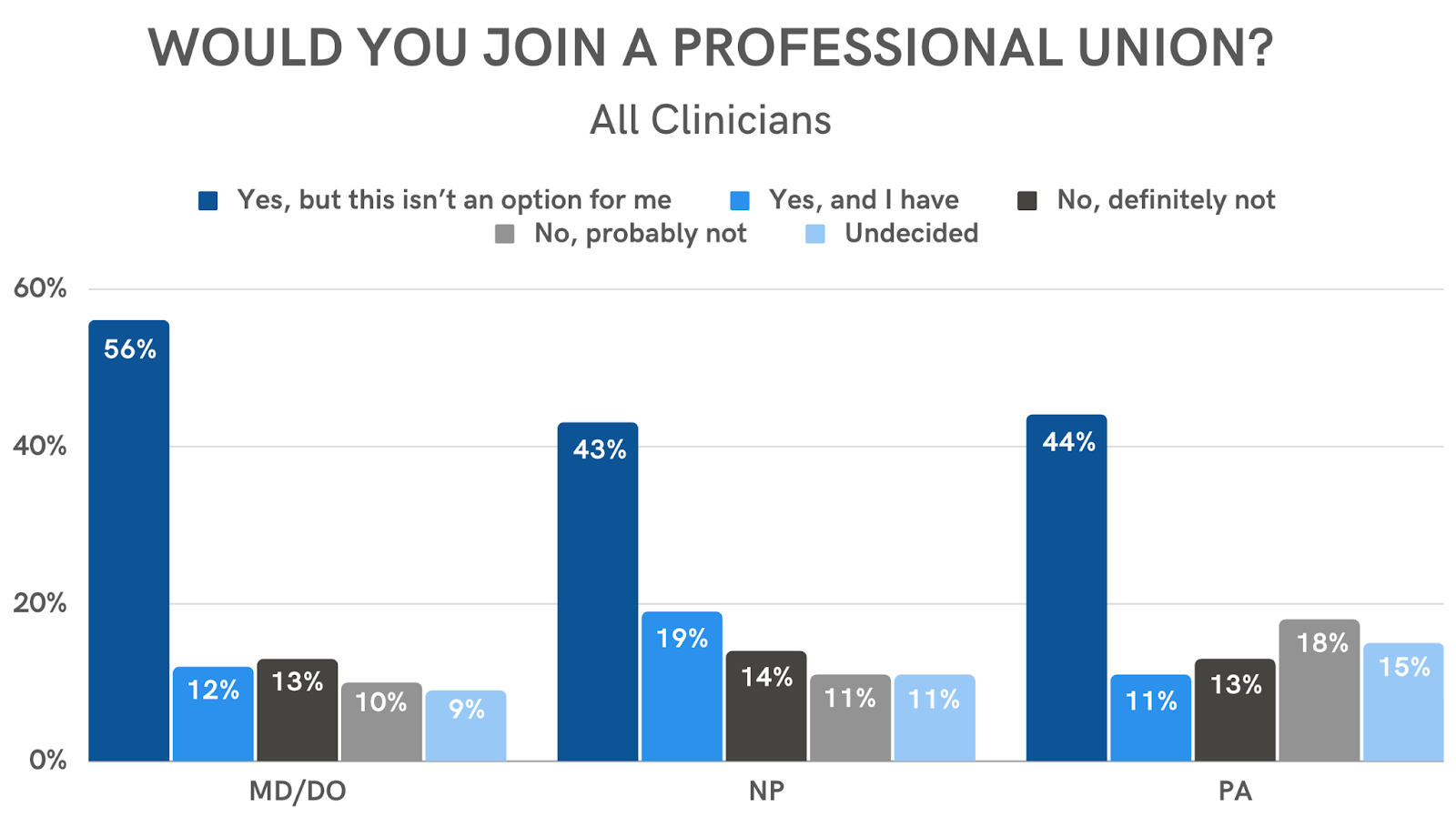
The poll included responses from more than 1,600 physicians, PAs, and NPs in November 2022. The majority of clinicians in each of these professions say they would join a union.
A higher percentage of physicians (68%) reported they would join a union or have already joined a union than NPs (62%) and PAs (54%). NPs had the highest percentage of clinician respondents (19%) who have already joined a union.
The results indicate broad interest in health care unions, which may signal potential changes for the industry.
“Widespread unionization could create a powerful coalition that could be used on behalf of our patients to tackle issues important to all of us, such as prior authorization and pharmacy benefit managers,” said Dr. Philip Seo, a rheumatologist and associate professor of medicine at the Johns Hopkins University School of Medicine, who detailed some of the possible benefits of unionization.
Younger clinicians appear to be more interested than older clinicians in unionization. Three-fourths of clinicians in their 30s are willing to join a union, a higher percentage compared to respondents in their 40s (64%), 50s (60%), 60s (60%), and 70s (44%).
Clinicians in their 20s, however, appear more hesitant, with only 57% of respondents willing to join a union. Of note, though only a small number of physician residents participated in the poll, 22 out of 23 say they are willing to join a union, with one undecided.
A higher percentage of women (66%) than men (59%) say they would join a union. And a higher percentage of women (14%) than men (11%) have, at some point, joined a union.
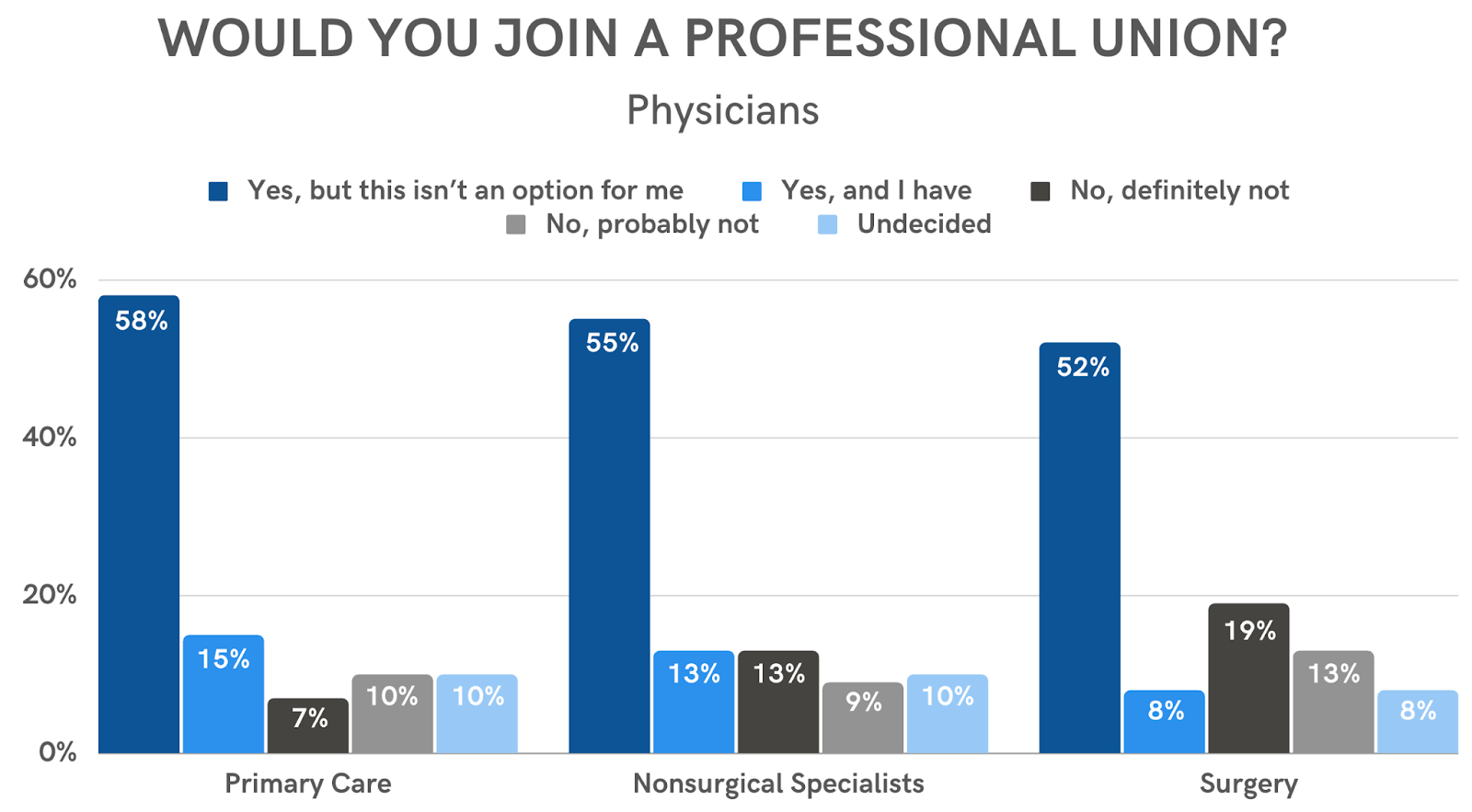
Among physicians polled, primary care physicians (73%) are more likely than surgeons (61%) to be interested in joining a union. Non-surgical specialists sit in the middle at 68%.
A potential explanation for the differing preferences by age, gender, and medical specialty is that older clinicians tend to hold higher positions and pay than younger clinicians, as is often the case for men versus women and surgeons versus PCPs. In turn, clinicians who earn less pay or hold a lower-level position may be more inclined to join a union.
Still, the overarching trend remains: Across all ages, genders, specialties, and professions, the majority of clinicians (64%) who responded to the poll say they are willing to join a union.
A Complex Issue
Ongoing concerns in medicine — from overwork to surging hospital and practice consolidation — seem to have renewed interest in unions over the past few years. Clinicians have recently appealed to colleagues to consider unionization, and an increasing number of residents have unionized each year since the start of the pandemic.
In the case of Dr. Jennifer Mushtaler, an ob/gyn in Texas who has seen these issues worsen over time, the response is clear. “The corporatization of medicine has often resulted in an environment in which physicians are subjected to dangerous work conditions and work hours, without the necessary support to do their jobs fully,” Dr. Mushtaler said. “Ultimately, if we continue to devalue physicians and our work, it will be our patients who suffer the consequences.”
Yet overall clinician willingness to unionize, based on the poll results, starkly contrasts current unionization rates among health care workers and the working population at large. The U.S. Bureau of Labor Statistics reported a union membership rate of 10.1% in 2022 — the lowest rate on record since it started tracking comparable data in 1983. Similarly, a study published in JAMA found that labor unionization among health care workers remained flat, at around 13.2%, from 2009-2021.
Despite their willingness, many clinicians find that joining a union is not an option in their current situation. The poll results showed that 51% of clinicians are willing to join a union but do not believe they are currently able to do so.
Narrow participation in unions stems in part from legislative restrictions. The National Labor Relations Act of 1935, for example, bars from unionization “any individual having the status of an independent contractor, or any individual employed as a supervisor.” The stipulation may apply to many clinicians working locum tenens and particularly to physicians, who are often considered managers or supervisors. Another policy, the Sherman Antitrust Act of 1890, also prohibits unionization agreements between businesses at the same level of the supply chain, which could potentially apply to those in private practice.
Perhaps a more immediate limitation for doctors is that many are unaware of the presence of local unions or how to join them, according to Dr. Seo.
“The biggest impediment to unionization is that individual physicians don't know where to begin,” he said. “In my career, I've never been approached by a union rep. If I wanted to join a physician union, I wouldn't know where to start.”
Dr. Seo suggested that physicians would likely need to take the initiative to move unionization forward — reaching out to local representatives in areas where relevant unions are present, or building a critical mass of local interest in areas where they are not.
Critics of unionization, in contrast, have expressed concern that the potential drawbacks may outweigh the benefits. Unionization entails ceding some autonomy to labor leaders and often involves mandated strikes, which could disrupt the patient-clinician relationship and negatively affect clinician reputation, noted Dr. Allan Dobzyniak, an internist working in Michigan.
“How is it possible for such a system to preserve the sanctity of the patient-to-physician relationship?” he said. “The answer is it cannot. And there will be another industry, labor, taking a bite of the apple.”
What’s more, Dr. Dobzyniak said that the medical community surrendered much of their marketplace freedom when they allowed payment to be determined by external companies and organizations, rather than by consumers. The situation may leave many without a clear sense of their value, which would be critical for leverage in union-driven negotiations.
“The allure of unionization as an easy way to solve complex issues will serve only to further identify physicians as employees for the ever-increasing managerial and political bureaucracies that have been able to wield increasing power over a profession that was never intended to forego its freedom and independence,” he said.
Nonetheless, Dr. Dobzyniak acknowledged the need for change. He suggested instead that the medical community invest first in educating future clinicians about the health care marketplace, basic business principles, finance, health care law, and the politics of medicine. In addition, he emphasized the importance of encouraging and nurturing the growth of strong, recognizable medical leaders.
“For the profession of medicine to maintain its identity as independent professionals devoted to the singular interest of each patient and acting without compromise to guard the patient-physician bond, change is necessary,” he said. “[But it] cannot be tweaked at the edges to salvage the profession.”