


Like many others, I entered one of the most challenging fields to date, so that one day I can learn to comprehend the human mind and body and provide care to the most innovative organism to set foot on this planet. Hence, I chose to study cell biology and neuroscience with psychology in my undergraduate years then went on to pursue my lifelong journey of learning medicine and completed my residency training in internal medicine and pediatrics. However, as my medical studies progressed, I became disillusioned, not only towards my ability to comprehend the vast amount of information required of me to care for the human body, and its intricacies along with the ever-evolving research, but also the business of health care.
It was during my second year of residency that the burnout caught up. I was ready to leave medicine and go into business school. I knew I wanted to go into primary care, but I could not fathom having to spend the rest of my life doing paperwork. It was while I was doing research on different practice styles for primary care medicine that I came across the concept of direct primary care. I traveled to Colorado that same year for a rotation at an organization that championed the principles of direct primary care. After my experience, I knew that I would pursue direct primary care after I completed my training.
In order to set myself up for success, I needed to learn about the existing health care system and its flaws. Like everyone else, I knew it was broken, but not how. After reading "Catastrophic Care" by David Goldhill and "America’s Bitter Pill" by Steven Brill, I had a better understanding of the existing health care system and its intricacies. I have since then concluded that the change required to fix the broken insurance-based primary care system and reverse primary care burnout isn’t complex and there is ample evidence for me to make that claim.
I, however, will not discuss the possible policy changes that can potentially reverse the path we have chosen to pursue, as there are many more intelligent people pursuing such answers. Instead, my focus is to analyze health care spending, primary care segmentation, physician burnout and allow you to decide whether the solution I discuss is a potential one.
Problem #1: Cost
One big problem with the insurance-based system is cost. Health care costs in the United States have increased significantly over the last decade, dramatically outpacing inflation at nearly three times the rate of inflation.
(Figure 1).
Problem #2: Burnout
Physician burnout has become widespread in our profession, likely driven by frustrating electronic health records, and soaring burden of administrative tasks all the while undermining patient encounters. Perhaps the catalyst to burnout and this new era of measurement and accountability that targets quality, errors, inequities, and soaring costs may be possibly due to the 1999 publication of the Institute of Medicine’s “To Err is Human” report or the implementation of the Affordable Care Act in 2010. Whatever the cause, the burnout is real, and patients do not like being cared for by physicians who are experiencing symptoms of burnout, which further translates to reduced patient satisfaction in primary care and increased medical errors.
Problem #3: Shortage
Since 2009, primary care visitation has been steadily dropping, according to data collected by the Health Care Cost Institute. The decrease has been especially sharp in recent years, as patients switch to lower-cost urgent care centers staffed with more nurse practitioners and physician assistants. 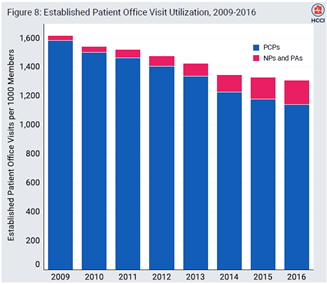

These problems, I believe, are the key to the continued destruction of primary care. The increasing cost of primary care has potentiated increasing control by the government by enforcing measurement and accountability which has further translated into a system of rewards, punishments, and pay-for-performance. This tightening control has led to increased burdens and administrative tasks alienating physicians, not only from direct patient engagement, the core of their desire to pursue medicine, but also from their families which has further potentiated burnout. Burnout overall contributes to a 1% reduction in physicians’ professional work effort, which equates to losing the graduates of seven medical schools annually — before accounting for other outcomes of burnout such as early retirement, leaving the profession altogether, and even physician suicide. This snowball effect will continue to destroy our primary care system. Even though many states have offered solutions such as providing nurse practitioners full practice rights so that they may serve the same role primary care physicians do, this solution will not fix the core of this problem, and the mounting stress among clinicians is likely to continue to increase burnout and cost. Replacing physicians will only shift the problem.
However, there is a solution, for cost control in primary care, to address physician burnout and to address the primary care shortage, and that solution, I believe, is direct primary care, which I will further discuss in my next article.
Adil Manzoor is an internal medicine/pediatric physician practicing in New Jersey. He's passionate about mentoring the next generation of leaders. In his free time he writes for local newspapers, mentors youth, reads voraciously, and most important of all, spends time with his wife and their daughter. And when time finally permits, binges Netflix! He can be found on Twitter at @Manzooradil2. Adil is a Doximity 2019-2020 Fellow.





